

Case Report
Testicular Torsion: Timely Diagnosis and Successful Salvage: A Case for Testicular Preservation
- Gurmeet Singh Sarla *
- Abhishek Kumar
General and Laparoscopic Surgeon, Department of Surgery, Military Hospital Khadki, Pune, Maharashtra, India.
*Corresponding Author: Gurmeet Singh Sarla, General and Laparoscopic Surgeon, Department of Surgery, Military Hospital Khadki, Pune, Maharashtra, India.
Citation: Sarla GS, Kumar A. (2026). Testicular Torsion: Timely Diagnosis and Successful Salvage: A Case for Testicular Preservation, International Journal of Biomedical and Clinical Research, BioRes Scientia Publishers. 6(2):1-5. DOI: 10.59657/2997-6103.brs.26.116
Copyright: © 2026 Gurmeet Singh Sarla, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: December 31, 2025 | Accepted: February 02, 2026 | Published: February 06, 2026
Abstract
Background: Testicular torsion is a urological emergency caused by twisting of the spermatic cord, leading to compromised blood flow and potential testicular loss if not promptly treated. Although commonly seen in adolescents, it can occur in adults, where timely diagnosis remains critical for testicular salvage.
Case Presentation: We report the case of a 31-year-old male who presented with acute onset left testicular pain of six hours’ duration. Clinical examination revealed an elevated, tender testis with absent cremasteric reflex, and a TWIST score of 6, strongly suggestive of testicular torsion. Colour Doppler ultrasonography demonstrated absent intratesticular blood flow with a characteristic whirlpool sign of the spermatic cord. Emergency scrotal exploration revealed a 360-degree torsion with a dusky, ischemic testis. Prompt detorsion followed by warm saline wrapping and oxygenation resulted in visible reperfusion within 15 minutes. Bilateral orchiopexy was performed. Postoperative Doppler ultrasonography confirmed preserved vascularity and viability of the affected testis.
Conclusion: This case highlights the importance of early clinical recognition, supportive use of Doppler ultrasonography, and prompt surgical intervention in achieving successful testicular salvage, even in adult patients presenting with absent preoperative blood flow.
Keywords: testicular torsion; diagnosis; doppler ultrasonography; case report
Introduction
Testicular torsion involves twisting of the spermatic cord, leading to obstruction of both arterial and venous blood flow. This vascular compromise results in testicular swelling, ischemia, and, if untreated, necrosis. Adolescent males are particularly vulnerable, with the most common underlying cause being the “bell clapper” deformity. In this condition, the tunica vaginalis fails to anchor the testis to the epididymis and posterior scrotal wall, allowing free rotation along its longitudinal axis-often affecting both testes. Testicular torsion is a urological emergency requiring rapid diagnosis and intervention to prevent irreversible damage. The primary goal is to restore arterial perfusion and minimize hypoxic injury to the testis [1].
Case Report
A 31-year-old male with no known comorbidities presented with a sudden onset of left testicular pain lasting six hours. The pain was acute, moderate in intensity, dull aching, constant, and non-radiating. It was associated with swelling of the left testis. The patient reported a history of heavy weight lifting and sexual activity one day prior to symptom onset. He denied any history of constipation, active sports, nausea, vomiting, fever, or lower urinary tract symptoms. There was no prior history of similar complaints, no relevant family history, and no previous surgical intervention involving the scrotum.
On General Examination
The patient appeared distressed but was oriented to time, place, and person. Vital signs were stable: temperature 98°F, respiratory rate 18/min, pulse 96/min, blood pressure 124/76 mmHg, and oxygen saturation 98% on room air.
Local Examination
Left hemiscrotum revealed swelling without erythema or dilated veins. The left testis was elevated, tender, non-fluctuant, and did not transilluminate.
Prehn’s sign and cremasteric reflex were absent on the affected side, while the right testis was normal.
TWIST Score-6(2).
Scrotal Doppler ultrasound
The left testis was normal in size and shape but showed a heterogeneous echotexture with absent vascularity on color Doppler. A minimal hydrocele was noted in the left hemiscrotum. Twisting of the cord structures was also observed at the superior aspect of the left testis, displaying a characteristic “whirlpool” appearance.
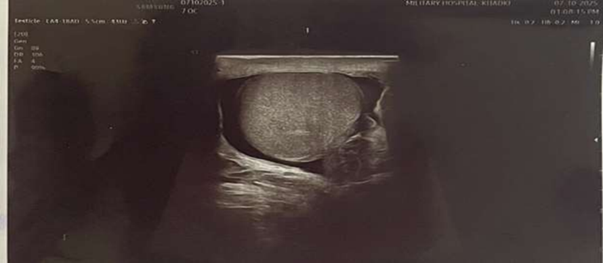
Figure 1: USG Scrotum showing absent testicular vascularity Secondary Hydrocele.
Intraoperatively, the left testis appeared dusky and ischemic, consistent with compromised perfusion. Detorsion was performed, and the testis was wrapped in a warm saline-soaked abdominal swab to promote reperfusion and patent was given 100% oxygen via face mask. After approximately 15 minutes, areas of vascular recovery were observed within the testis. Given the restoration of blood flow, bilateral orchiopexy was performed to prevent future torsion.

Figure 2: Intraoperative image - congested, enlarged, bluish, and hemorrhagic testis with twisted spermatic cord.

Figure 3: Intraoperative image showing testis after detorsion of spermatic cord.

Figure 4: Intraoperative image showing testis after 15 min of oxygenation and warm saline.

Figure 5: Intraoperative image, comparing both testes.

Figure 6: Intraoperative image, comparing both testes after 15 min of oxygenation and warm saline.
Follow-Up Scrotal Ultrasonography After Orchidopexy
Both testes showed normal shape, size, and echotexture with no focal lesions identified. The left epididymis appeared mildly enlarged, while the right epididymis was normal. Increased vascularity was noted in the left testis and epididymis. The pampiniform plexus was visualized normally, and no abnormal fluid collection was seen. Overall findings were suggestive of a viable left testis with preserved vascularity and postoperative changes, with no evidence of recurrent torsion or ischemia.

Figure 7: USG left testis post op.

Figure 8: USG Right testis post op.
Discussion
Testicular torsion is a surgical emergency that requires prompt diagnosis and intervention to prevent irreversible damage. The TWIST (Testicular Work-up for Ischemia and Suspected Torsion) score was developed to allow for expedited diagnosis of testicular torsion (TT) in children based on clinical variables: edema (2 points), hard mass (2), absent cremasteric reflex (1), high-riding testis (1) and nausea/vomiting (1). The TWIST Score is valid for the diagnosis of Testicular Torsion in adults, presenting a PPV of 90% for a cutoff of 5 points and 100% for six points. In all patients with a score of 2 or less, the disease could be safely excluded (100% NPV) [2].
Doppler ultrasound is a valuable diagnostic tool, often revealing absent or reduced blood flow to the affected testis. Once torsion is suspected, immediate surgical exploration is warranted [3]. Testicular survival when surgically managed at 0 to 6 hours from symptom onset is found to be 95.7%, 7 to 12 hours, 77.8%; 13 to 24 hours, 49.2%; 25 to 48 hours, 29.2% and only 9.6% with greater than 48 hours delay [4].
During the procedure, the testis is assessed for viability—if it appears dusky or ischemic, detorsion is performed, and the testis may be wrapped in warm saline-soaked gauze to encourage reperfusion. In some cases, an incision into the tunica albuginea may be made to relieve pressure and further evaluate tissue viability. For patients presenting late, careful intraoperative assessment is essential to determine whether the testis can be salvaged. Regardless of the outcome on the affected side, the contralateral testis should be explored and fixed (orchidopexy) due to the high risk of bilateral torsion, especially in cases involving anatomical predispositions like the bell clapper deformity [3].
Although our patient had symptoms for approximately 8 hrs with absent flow on DUS, it was timely diagnosis and surgical intervention which had led to successful salvage of testis.
In addition, the degree of torsion also impacts the viability of the testicle. It was found that patients undergoing orchiopexy had a median of 360 degrees of torsion with a median of 12 hours of symptoms, while patients undergoing orchiectomy experienced a median of 540 degrees of torsion with a median of 90 hours of symptoms [5]. Our patient was found to have 360 degrees of torsion at the time of surgical detorsion which may also have contributed to salvageability of the testicle and decision to perform a bilateral orchiopexy instead of an orchiectomy.
Conclusion
To optimize testicular viability, immediate surgical intervention is essential once torsion is suspected. While clinical guidelines suggest timeframe for 6 hours for viability—individualized assessment remains crucial, as salvageability may still be possible beyond these limits. Intraoperatively, the affected testis may appear dusky, edematous, or ischemic. Detorsion is performed, and the testis is often wrapped in warm saline-soaked gauze to promote reperfusion. In some cases, an incision into the tunica albuginea may be made to relieve compartment pressure and assess viability more accurately. If signs of perfusion return, orchidopexy is performed to secure the testis. Regardless of viability, the contralateral testis should also be explored and fixed due to the risk of bilateral torsion, especially in patients with anatomical predispositions such as the bell clapper deformity.
Take Home Message
- Testicular torsion is a surgical emergency-clinical suspicion alone is sufficient to proceed to urgent scrotal exploration without delay.
- Preoperative Doppler findings do not definitively determine testicular viability; the final decision should be based on intraoperative assessment.
- Immediate detorsion, warm saline application, and oxygenation are effective intraoperative measures to promote reperfusion of a compromised testis.
- Testicular salvage is possible beyond the traditional 6-hour window, particularly with lower degrees of torsion and prompt surgical intervention.
- Bilateral orchiopexy should be routinely performed, regardless of the affected side, to prevent future torsion in patients with anatomical predisposition.
References
- Cios K, Kohn D, Hall P, Mishail A, Louis M. (2023). Testicular Torsion, Time Is of The Essence: A Case for Testicular Preservation. Int Surg J. 10(7):1220-122.
Publisher | Google Scholor - Barbosa, J. A. B. A., de Freitas, P. F. S., Carvalho, S. A. D., Coelho, A. Q., Yorioka, M. A. W., et al. (2021). Validation of The TWIST Score for Testicular Torsion in Adults. International Urology and Nephrology, 53(1):7-11.
Publisher | Google Scholor - O'Connell, P. R., McCaskie, A. W., Sayers, R. D. (2023). Bailey & Love's Short Practice of Surgery- 28th Edition, CRC Press.
Publisher | Google Scholor - Zhao, L. C., Lautz, T. B., Meeks, J. J., Maizels, M. (2011). Pediatric Testicular Torsion Epidemiology Using a National Database: Incidence, Risk of Orchiectomy and Possible Measures Toward Improving the Quality of Care. The Journal of Urology, 186(5):2009-2013.
Publisher | Google Scholor - Brenner, J. S., Ojo, A. (2015). Causes of Scrotal Pain in Children and Adolescents. UpToDate.
Publisher | Google Scholor























