

Review Article
Synovial Fluid Function in the Knees
1 Department of Chemistry Sri Sharda Group of Institutions Lucknow U.P. India.
2 Department of Chemistry Dayanand Girls P.G. College Kanpur U.P. India.
*Corresponding Author: D.K. Awasthi, Department of Chemistry Sri Sharda Group of Institutions Lucknow U.P. India.
Citation: Awasthi D.K., Dixit A. (2025). Synovial Fluid Function in the Knees, Clinical Case Reports and Studies, BioRes Scientia Publishers. 11(1):1-4. DOI: 10.59657/2837-2565.brs.25.286
Copyright: © 2025 D.K. Awasthi, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: October 21, 2025 | Accepted: November 04, 2025 | Published: November 11, 2025
Abstract
Synovial fluid is a specialised viscous fluid within the knee (and other synovial joints) that enables near-frictionless motion, distributes load, cushions impact, and supplies nutrients to avascular articular cartilage. Its unique rheological and biochemical properties arise from macromolecules such as high–molecular-weight hyaluronan (hyaluronic acid), surface-active glycoproteins (lubricin/PRG4), and phospholipids. Alterations in composition and rheology contribute to joint pain and degeneration (e.g., osteoarthritis, inflammatory arthritis). This review summarizes the composition, mechanical and biological roles, disease-related changes, and clinical implications (diagnosis and treatment) with representative images and primary references.
Keywords: synovial fluid; knee; hyaluronan; lubricin (prg4); lubrication; cartilage nutrition; arthrocentesis; viscosupplementation
Introduction
The knee is a large synovial joint whose articular surfaces are covered with avascular hyaline cartilage. The synovial membrane (synovium) lines the joint capsule and produces synovial fluid (SF) — an ultrafiltrate of plasma enriched with macromolecules that give SF its lubricative and shock-absorbing functions. SF is central to joint homeostasis and is a diagnostic window into joint pathology.
Composition of Synovial Fluid
Major components and their roles:
- Water (≈90%) — solvent and transport medium
- Hyaluronan (HA; hyaluronic acid) — very high molecular weight glycosaminoglycan responsible for SF viscosity and non-Newtonian rheology; provides boundary and elastohydrodynamic lubrication under load. HA concentration and molecular weight strongly influence lubrication.
- Lubricin (Proteoglycan 4, PRG4) — a surface-active glycoprotein that adsorbs to cartilage surfaces and reduces friction, particularly in boundary lubrication regimes.
- Surface-active phospholipids and lipids — contribute to the surface film on cartilage and help keep friction low under certain conditions.
- Cells and solutes — synoviocytes, a small number of leukocytes, electrolytes, proteins (albumin, globulins), enzymes and cytokines; composition shifts markedly in disease (inflammation, infection).
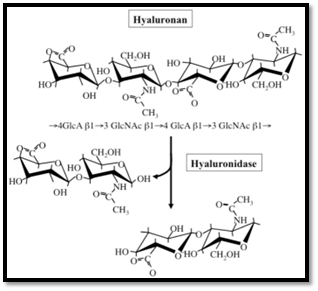
Figure 1: chemical structure of hyaluronan shown above
Mechanical / Biomechanical Functions
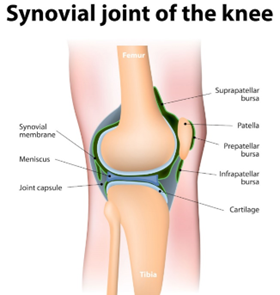
Figure 2: Lubrication
SF provides several complementary lubrication mechanisms:
- Boundary lubrication: lubricin and adsorbed molecules form a thin layer on cartilage surfaces that directly lowers friction during slow/sliding contact
- Fluid film / elastohydrodynamic lubrication: under rapid loading, viscous HA helps maintain a thin fluid film between cartilage surfaces, reducing contact stresses. The combined action of HA, lubricin and phospholipids is crucial for low friction under high loads.
Shock absorption and load distribution
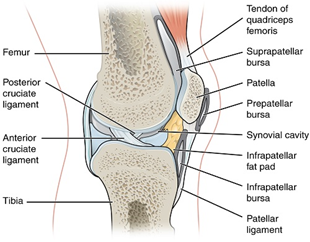
Figure 3: Synovial fluid cavity
SF and the pressurisation of interstitial water in cartilage help distribute compressive loads and protect cartilage from focal overload. Rheological properties (viscosity, shear thinning) are optimized to change with loading rate.
Wear reduction
By reducing friction and spreading loads, SF minimizes wear of the articular surface and delays degenerative changes. Experimental models show synergistic effects of HA + lubricin + phospholipids in reducing cartilage wear
Biological / Nutritional Roles
Articular cartilage is avascular — chondrocytes rely on diffusion from SF for oxygen, glucose, and metabolite exchange. Normal SF turnover and composition are therefore essential for cartilage metabolism and repair. Disturbances (inflammation, reduced HA) impair nutrient transport and waste removal, contributing to degeneration
Changes in Disease
Osteoarthritis (OA)
OA SF often shows reduced HA molecular weight and concentration, reduced lubricin function, altered phospholipid content, and increased pro-inflammatory mediators. These changes reduce viscosity and lubrication efficiency, increasing friction and cartilage damage progression.
Inflammatory arthritides (e.g., RA)
Inflammation increases cell count, protein, cytokines, and enzymes in SF — often lowering viscosity and altering composition (hyaluronidase release cleaves HA). Synovial inflammation drives joint destruction if uncontrolled. SF analysis helps differentiate inflammatory vs non-inflammatory vs septic processes.
Septic arthritis / crystal arthropathies
Infection produces purulent, highly cellular SF with low glucose and high neutrophil counts. Crystal-induced arthritis (gout/pseudogout) is diagnosed by polarized light microscopy of aspirated SF. Arthrocentesis (aspiration) is both diagnostic and sometimes therapeutic.).
Clinical Implications
Diagnosis — Synovial fluid analysis
Arthrocentesis (joint aspiration) is an essential diagnostic tool when there is effusion, acute monoarthritis, suspected infection, or unclear inflammatory cause. Analysis includes appearance, cell count/differential, Gram stain/culture, crystal analysis, glucose, protein, and sometimes HA assessment.
Therapeutic approaches related to synovial fluid
- Viscosupplementation (intra-articular hyaluronic acid): aims to restore viscoelastic properties of SF and reduce pain in OA; clinical efficacy varies by product and patient selection
- Injections (corticosteroids, PRP, biologics): modify the synovial environment to reduce inflammation and pain; choice depends on diagnosis.
- Arthrocentesis: relieves painful effusion and allows diagnostic testing.
Research Directions & Biomimetics
Understanding the cooperative action of HA, lubricin and lipids has informed biomimetic lubrication strategies and engineered lubricants for joint therapy and prosthetic surfaces. Ongoing work explores HA molecular weight optimisation, PRG4 supplementation, and combined formulations to mimic native SF.
Conclusion
providing lubrication, shock absorption, nutrient delivery and a milieu that maintains cartilage health. Disease-related alterations to SF composition and rheology are central to joint pain and degeneration; thus, both diagnostic analysis and therapeutic strategies often target SF properties (e.g., viscosupplementation, modulation of inflammation). Continued research into molecular lubrication and biomimetic replacements holds promise for future treatments.
References
- Seidman, A. J., et al. (n.d.). Synovial fluid analysis. In StatPearls.
Publisher | Google Scholor - Tamer, T. M. (n.d.). Hyaluronan and synovial joint: Function, distribution, and roles. PubMed Central (PMC).
Publisher | Google Scholor - Temple-Wong, M. M., et al. (2016). Hyaluronan concentration and size distribution in human synovial fluid: Variations with age and osteoarthritis. PubMed Central (PMC).
Publisher | Google Scholor - Giarritiello, F. (2025). Viscosupplementation and synovial fluid rheology. PubMed Central (PMC).
Publisher | Google Scholor - An, H., et al. (2022). Research progress of cartilage lubrication and biomimetic materials. Frontiers in Bioengineering and Biotechnology.
Publisher | Google Scholor - Krakowski, P., et al. (2024). Cartilage integrity: A review of mechanical and frictional properties of articular cartilage. MDPI.
Publisher | Google Scholor - Blewis, M. E., et al. (n.d.). A model of synovial fluid lubricant composition and its relation to joint function. Extracellular Matrix (ECM) Journal.
Publisher | Google Scholor - Practical and educational resources on arthrocentesis and synovial fluid analysis. (n.d.). Physiopedia; Labpedia.
Publisher | Google Scholor























