

Case Report
Severe Hypocalcemia Causing Acute Heart Failure Decompensation with Exacerbation of Mitral and Tricuspid Regurgitation
1 Department of Cardiology, Bahman University Hospital, Beirut, Lebanon.
2 Internal Medicine, Bahman Hospital, Beirut, Lebanon.
3 Pulmonary and Critical Care, Balamand University, Beirut, Lebanon.
4 Department of Nephrology, Bahman Hospital, Beirut, Lebanon.
5 Cardiovascular Disease, Bahman Hospital, Beirut, Lebanon.
*Corresponding Author: Hasan Kazma, Department of Cardiology, Bahman University Hospital, Beirut, Lebanon.
Citation: Kazma H., Nina H., Khalil M., Mollaei S., Jibai A. (2025). Severe Hypocalcemia Causing Acute Heart Failure Decompensation with Exacerbation of Mitral and Tricuspid Regurgitation, Journal of BioMed Research and Reports, BioRes Scientia Publishers. 9(1):1-9. DOI: 10.59657/2837-4681.brs.25.216
Copyright: © 2025 Hasan Kazma, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: November 03, 2025 | Accepted: November 17, 2025 | Published: November 25, 2025
Abstract
Hypocalcemia can lead to arrhythmias and to left ventricular dysfunction. We present herein this case of a 93 years old man with multiple myeloma (MM) who developed severe hypocalcemia secondary to treatment with Zoledronic acid. The severe hypocalcemia induced by Zoledronic acid led to acute decompensation of stable heart failure (HF) and to an increase of the mitral and tricuspid regurgitation severity with pulmonary edema requiring intubation, mechanical ventilation and inotropic support. Correction of the hypocalcemia using intravenous calcium gluconate reversed the cardiac decompensation and improved the mitral and tricuspid regurgitation as demonstrated by transthoracic echocardiography, with an improvement in the clinical condition of the patient.
Keywords: hypocalcemia; heart; mitral and tricuspid regurgitation
Introduction: Case Presentation
This is a 93 years old man with long standing history of congestive heart failure (CHF) and reduced ejection fraction (EF) at 30%, coronary artery disease (CAD) with a history of coronary artery bypass grafting (CABG) twenty years ago and a history of percutaneous coronary intervention (PCI) to the diagonal artery branch of the left anterior descending (LAD) artery seven years ago, chronic kidney disease (CKD), diabetes mellitus (DM) , dyslipidemia and MM for which he was treated with intravenous Bortezomib plus dexamethasone cycles, subcutaneous erythropoietin and packed RBC transfusion as required. His medication consisted of: Bisoprolol 2.5 mg orally daily, spironolactone 25 mg orally daily, Empagliflozin 10 mg orally daily, Ramipril 2.5 mg orally daily, Furosemide 60 mg orally daily, Atorvastatin 20 mg orally daily and Linagliptin 5 mg orally daily. The timeline of patient’s medical conditions with the treatment offered is depicted in table 1.
Table 1: Table 1 depicts the timeline of patient’s medical conditions with the treatment offered
| Disease | Date of onset | Treatment |
| Dyslipidemia | 20 years ago | Atorvastatin 20 mg orally |
| CAD | 20 years ago | CABG |
| Unstable angina | 7 years ago | PCI of the diagonal branch of the LAD artery. |
| Diabetes mellitus | 7 years ago | Linagliptin 5 mg orally daily. |
| Empagliflozin 10mg orally daily. | ||
| CHF | 3 years ago | Bisoprolol 2.5 mg orally daily. |
| Spironolactone 25 mg orally daily. | ||
| Empagliflozine 10 mg prally daily. | ||
| Ramipril 2.5 mg orally daily. | ||
| Furosemide 60mg orally daily. | ||
| CKD | 3 years ago | Empagliflozin 10 mg orally daily |
| Ramipril 2.5 mg orally daily | ||
| Multiple myeloma | 2 years ago | Intravenous bortezomib plus dexamethasone cycles on weekly basis. |
| Sub cutaneous erythropoietin and packed RBC transfusion as required. |
CAD=coronary artery disease; CABG=coronary artery bypass grafting; PCI=percutaneous coronary intervention; CHF=congestive heart failure; LVEF=left ventricular ejection fraction. CKD=chronic kidney disease.
Patient received Zoledronic acid to treat severe osteoporotic lesions of the lumbar vertebrae leading to multiple fractures (3rd and 4th lumbar vertebrae) and causing severe pain despite analgesics and a kyphoplasty of 4th lumbar vertebrae (L4); The oncologist recommended Zoledronic acid to prevent further episodes of fractured Lumbar vertebrae; after treatment with Zoledronic acid the patient was observed for 4 days in hospital and then discharged home; the calcium, phosphorus, magnesium, creatinine, electrolytes and albumin levels four days after zoledronic acid treatment were all normal (table 2); during this admission, patient was in New York heart association (NYHA) II classification of heart failure, his left ventricular (LV) ejection fraction (EF) was reported at 30%.
Table 2: Laboratory results showing calcium. phosphorus, magnesium, creatinine, electrolytes and albumin levels four days after Zoledronic acid treatment.
| Laboratory results | 4 days after Zoledronic acid treatment | Normal range |
| Calcium mg/dl | 8.6 | 8.5-10.5 |
| Phosphorus mg/dl | 3.1 | 2.5-4.4 |
| Magnesium g/dl | 2.1 | 1.5-2.5 |
| Creatinine mg/dl | 1.28 | 0.7-1.3 |
| Sodium meq/l | 133 | 135-145 |
| Potassium meq/l | 4.4 | 3.5-5.0 |
| Chloride meq/l | 96 | 96-106 |
| CO2 meq/l | 26 | 22-28 |
| Albumin g/l | 41 | 3.5-5 |
He presented to our emergency room (ER) three days post discharge from our hospital (seven days after zoledronic acid treatment) with severe dyspnea tachypnea at rest and hypoxemia plus hypotension (blood pressure at 75 / 55mm Hg); he was intubated with mechanical ventilation using continuous mandatory ventilation (CMV) mode, sedated using intravenous (IV) midazolam plus fentanyl (midazolam at the dose of 3mg/hour IV and fentanyl at a dose of 150microgram/hour IV) and supported with inotropes (Dobutamine at the dose of 3 microgram/kilogram/minute and Noradrenaline at the dose of 0.5 microgram/minute); his ECG showed LBBB and there was no ECG changes compared to previous ECG (Figure 1). He was admitted to the intensive care unit.
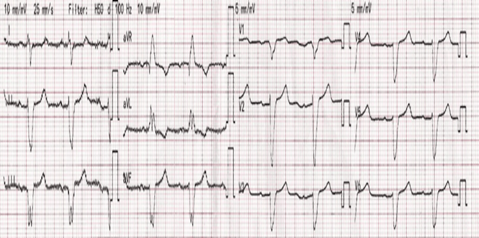
Figure 1: Electrocardiogram (ECG) showing left bundle branch block.
His Chest x ray (Figure 2 ) showed pulmonary edema and cardiomegaly.
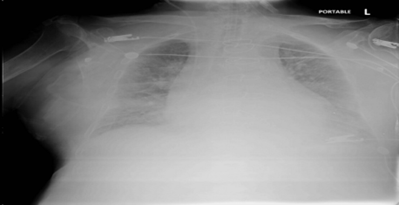
Figure 2: Chest x ray showing cardiomegaly and pulmonary edema.
Echocardiography done urgently, while patient was receiving inotropic support, and showed a reduced LVEF at 19% (Figure 3).
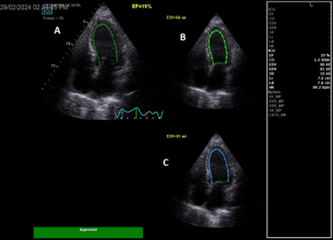
Figure 3: A: Apical 4 chambers view showing automatic left ventricular ejection fraction at 19%. B: LV end systolic volume at 66ml. C: LV end diastolic volume at 81ml.
LA=left atrium; LV=left ventricle; RA=right atrium; RV=right ventricle; EF=ejection fraction; ESV = end systolic volume; EDV = end diastolic volume.
Color Doppler mapping of the mitral valve showed severe mitral regurgitation (MR) (Figure 4).
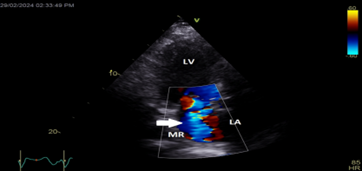
Figure 4: Apical long axis view still frame showing severe mitral regurgitation (white arrow)
LA=left atrium; LV=left ventricle; MR=mitral regurgitation
Color Doppler mapping of the tricuspid valve showed severe tricuspid regurgitation (TR) (Figure 5).
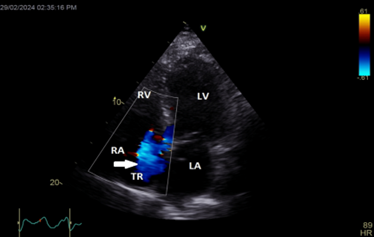
Figure 5: Apical 4 chambers view showing severe tricuspid regurgitation (white arrow).
LA=left atrium; LV=left ventricle; RA=right atrium; RV=right ventricle; TR=tricuspid regurgitation
Continuous wave (CW) Doppler interrogation of the tricuspid regurgitant jet yielded a jet velocity at 3.85 m/sec allowing calculation of systolic pulmonary artery pressure( SPAP) at 67 mmHg with estimated right atrial pressure at 8 mmHg (Figure 6); the inferior vena cava was normal in size at 1.6 cm and collapsing normally with inspiration.
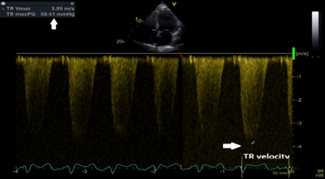
Figure 6: CW Doppler interrogation of the tricuspid regurgitant jet yielded a jet velocity at 3.85 m/sec (white arrows) allowing calculation of SPAP at 67 mmHg with estimated right atrial pressure at 8 mmHg; the inferior vena cava was normal in size at 1.6 cm and collapsing normally with inspiration.
CW=continuous wave Doppler; m/s=meter/second; SPAP=systolic pulmonary artery pressure.
Blood test showed a calcium level of 4.3 mg/dl (normal level is from 8.5-10.5 mg/dl) and albumin level of 33 mg/dl (normal level 35-50 g/l) indicating a severe drop of free calcium because the albumin level was normal. Immediate intravenous calcium replacement was done: calcium gluconate at the dose of 300mg in 50 cc D5W was given urgently intravenously over 30 minutes then an intravenous drip of calcium gluconate was started at 1mg/kg/hour using an electric pump; the aim was to reach a low normal blood level of calcium at 8-8.4 mg/dl; Noradrenalin at the dose of 0.5 microgram/minute and Dobutamine at the dose of 3 microgram/kilogram/minute were continued. On the third day the calcium level increased to 7.4mg/dl (Table 3) and patient condition improved markedly. his blood pressure improved 110 / 70 mmHg so continuous intravenous furosemide at the dose of 120 mg/24 hours by electric pump was started; on the 4th day the Ca level was 8 mg/dl, and patient was weaned off inotropes, sedation and mechanical ventilator (patient was extubated) with stable blood pressure at 110/65 mmHg, improved arterial blood gases (ABG’s) and a saturation at 98% with oxygen delivered via nasal cannula at 1.0 liter/minute (table 3). Table 3 summarizes the blood test of the patient and it shows the correction, over four consecutive days, of serum calcium using intravenous calcium gluconate, also it shows the improvement of ABG's of the patient after extubation on the day four of admission (Table 3).
Table 3: Shows creatinine, electrolytes, calcium, albumin, phosphorus, magnesium, TSH, PTH and vitamin D level, and ABG's during the correction of hypocalcemia (PaO2 measures the partial pressure of oxygen in arterial blood, while PaCO2 measures the partial pressure of carbon dioxide in arterial blood).
| Laboratory result | 3 days before discharge | 2 days before discharge | 24 hours before discharge | Normal range |
| Creatinine mg/dl | 1.38 | 1.18 | 1.28 | 0.7-1.3mg/dl |
| BUN mg/dl | 56 | 29 | 37 | 7-20mg/dl |
| Na meq/l | 134 | 134 | 133 | 135-145 meq/L |
| K meq/l | 3.7 | 4 | 4.4 | 3.5-5 meq/L |
| Cl meq/l | 97 | 99 | 96 | 96-106 meq/L |
| CO2 meq/l | 27 | 24 | 26 | 22-28 meq/L |
| Calcium mg/dl | 9.0 | 9.0 | 8.6 | 8.5-10.5 mg/dl |
| Albumin mg/dl | 41 | (-) | (-) | 3.5-5 g/dl |
| Globulin mg/dl | 26 | (-) | (-) | 2.0-2.5 g/dl |
| Phosphorus mg/dl | 3.8 | 4.2 | 3.1 | 2.5-4.4 mg/dl |
| Magnesium mg/dl | 3.08 | 2.41 | 2.1 | 1.5-2.5 mg/dl |
| HT % | 24.7 | 29.5 | 10.3 | 38.3-55 |
| Hb g/dl | 8.7 | 10.7 | 30.2 | 13.2-17.5 |
| WBC / microl | 6980 | 9430 | 9220 | 4500-11000 |
| Neutrophiles % | 90.2 | 86.4 | 85.2 | 40-60 |
| Lymphocytes % | 5.47 | 6.46 | 6.44 | 20-40 |
| Monocytes % | 3.93 | 6.44 | 7.14 | 4-8 |
| Platlets / microl | 136000 | 141000 | 124000 | 140-450000 |
| PaO2 mmHg | 96 | 83 | 97 | 75-100 |
| PaCO2 mmHg | 37 | 43 | 36 | 35-45 |
| Saturation % | 99 | 97 | 98 | 95-100 |
| PH | 7.5 | 7.48 | 7.45 | 7.35-7.45 |
TSH=thyroid stimulating hormone; PTH=parathyroid hormone; Vit D25_OH=25 hydroxy vitamin D level
Table 4 shows the results of cardiac troponin I level during the first four days of admission; it was slightly elevated on admission and returned to normal the next day. The changes in cardiac troponin I level at presentation was attributed to the hypotension and not to acute coronary syndrome.
Table 4: Shows the cardiac troponin I level on admission and in the next four days.
| Cardiac troponin I level | First day | Second day | Third day | Fourth day | Normal cTnI |
| cTnI ng/ml | 0.057 | 0.038 | 0.024 | 0.015 | < 0> |
After the 4th day intravenous calcium gluconate was stopped and patient was started on oral calcium carbonate (Caltrate) at a dose of 600mg every 6 hours orally with 1,25 hydroxy vitamin D (One-Alfa at a dose of 1 microgram daily orally) with a target Calcium level at 8-8.4mg/dl; also, intravenous furosemide was changed to oral furosemide at a dose of 100 mg orally daily. Repeat echocardiography after extubation and after weaning off inotropes showed an improvement in LVEF at 32% (Figure 7).
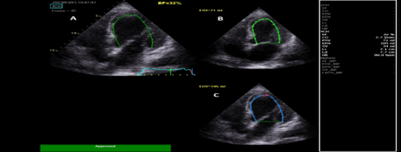
Figure 7: A: Apical 4 chambers view after correction of hypocalcemia showing a left ventricular ejection fraction at 32%. B: LV end systolic volume at 71ml; C: LV end diastolic volume at 105ml
LA=left atrium; LV=left ventricle; RA=right atrium; RV=right ventricle; EF=ejection fraction; ESV=end systolic volume; EDV= end diastolic volume.
Color Doppler mapping of the mitral valve showed a decrease in MR severity with only grade I mitral regurgitation noted after correction of hypocalcemia (figure 8).
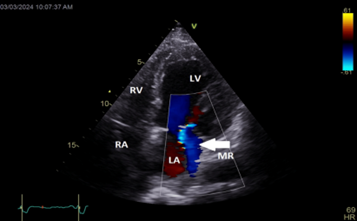
Figure 8: Apical 4 chambers view showing the decrease in mitral regurgitation severity (white arrow) after correction of hypocalcemia. LA=left atrium; LV=left ventricle; RA=right atrium; RV=right ventricle; MR=mitral regurgitation
Color Doppler mapping of the tricuspid valve showed a decrease in TR with only grade I tricuspid regurgitation noted after correction of hypocalcemia (Figure 9).
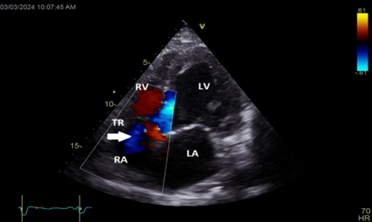
Figure 9: Apical 4 chambers view showing decrease of the tricuspid regurgitation severity (white arrow) after correction of hypocalcemia. LA=left atrium; LV=left ventricle; RA=right atrium; RV=right ventricle; TR=tricuspid regurgitation.
CW interpretation of the tricuspid regurgitant jet showed a decrease in TR velocity at 3.09 m/sec and thus an improvement of the SPAP at 43.1 mmHg with estimated RA pressure at 5 mmHg after correction of the hypocalcemia (figure 10).
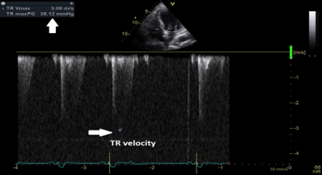
Figure 10: Continuous wave doppler interpretation of the tricuspid valve showing a decrease of the tricuspid regurgitant velocity (white arrows) at 3.09 m/sec; with a subsequent decrease of systolic pulmonary artery pressure at 43.1 mmHg. TR velocity=Tricuspid regurgitation velocity
All cultures including blood cultures deep tracheal aspirate (DTA) cultures and urine cultures taken during this admission were negative. Patient’s HF medications were restarted in the few days that followed. He was also started on oral calcium and active vitamin D (1.25 hydroxy vitamin D); with monitoring of serum calcium level and a target of calcium level at around 8-8.4mg/dl, he was discharged home 3 weeks after presentation to ER. Before discharge from hospital (after 3 weeks) patient was in stable clinical condition not requiring oxygen therapy and was able to ambulate unassisted.
Discussion
Our patient was a very elderly man with CKD and CHF, he was treated with guideline directed medical therapy for heart failure (the four pillars): angiotensin converting enzyme inhibitor (ramipril), beta blocker (bisoprolol), mineralocorticoid antagonist (spirolnolactone) and sodium glucose co-transporter inhibitor 2 (empagliflozin); he also had multiple myeloma and severe bone pain related to vertebral fracture that was refractory to analgesics and kyphoplasty so treatment with zoledronic acid was advised by the oncologist to prevent further bone fracture in vertebral bodies of the spine [8], this treatment led to severe hypocalcemia [2] and acute cardiac decompensation with reduction in LVEF from 30% to 19% during hypocalcemia, LVEF improved to 32
Conclusion
Intravenous use of bisphosphonate in patients with malignancies and bone involvement may lead to acute severe hypocalcemia. Patients at risk to develop hypocalcemia should be identified before the drug is administered and should be monitored carefully after treatment and given calcium and vitamin D (active form or 25 hydroxy calciferol). Severe acute hypocalcemia secondary to intravenous bisphosphonate can cause acute HF, so it should be recognized and treated very early since early intravenous calcium administration will prevent and even reverse the acute HF or the decompensation of already established stable HF. Functional mitral and tricuspid regurgitation will increase with the decompensated HF leading to exaggeration of symptoms and Guideline-directed drug therapy (GDMT)remains the first-line treatment for functional regurgitation across all HF phenotypes, followed by cardiac resynchronization therapy (CRT) in appropriately selected patients. Behind GDMT and CRT, surgical or trans-catheter valve therapy is a valuable option for patients remaining symptomatic. Pharmacological and non-pharmacological treatments are complementary and can interrupt valvar-driven HF progression in appropriately selected patients; however, when acute or subacute hypocalcemia develops due to other non-cardiac therapies the patient is receiving and leads to acute heart failure exacerbation with increase in valvar regurgitation, then correction of hypocalcemia should be done urgently first to see if it reverses the acute HF exacerbation. In conclusion, severe hypocalcemia as a possible cause of heart failure should be considered in the differential diagnosis of all individuals with congestive heart failure. The correction of serum calcium level results in the improvement of heart function and electrical activity.
References
- Tinawi, M. (2021). Disorders of calcium metabolism: Hypocalcemia and hypercalcemia. Cureus, 13(1):e12420.
Publisher | Google Scholor - Eisner, D. A., Caldwell, J. L., Kistamás, K., & Trafford, A. W. (2017). Calcium and excitation–contraction coupling in the heart. Circulation Research, 121(2):181–195.
Publisher | Google Scholor - Baqi, D., Ahmed, S., Baba, H., et al. (2022). Hypocalcemia as a cause of reversible heart failure: A case report and review of the literature. Annals of Medicine and Surgery, 74: 103572.
Publisher | Google Scholor - da Silva Santos, T., & de Carvalho, A. C. (2022). Hypocalcemic cardiomyopathy: A rare and reversible entity. The American Journal of Emergency Medicine, 51:426.e1–426.e2.
Publisher | Google Scholor - Jafari Fesharaki, M., Ahmadi, N., & Karimi Taheri, K. (2021). Reversible heart failure in a patient with hypocalcemic cardiomyopathy. Journal of Geriatric Cardiology, 18:1063–1067.
Publisher | Google Scholor - Gupta, P., Tomar, M., Radhakrishnan, S., & Shrivastava, S. (2011). Hypocalcemic cardiomyopathy presenting as cardiogenic shock. Annals of Pediatric Cardiology, 4(2):152–155.
Publisher | Google Scholor - Parepa, I., Mazilu, L., Suceveanu, A., Voinea, C., & Tica, I. (2019). Hypocalcemic cardiomyopathy: A rare heart failure etiology in adults. Acta Endocrinologica (Bucharest), 15(1):107–112.
Publisher | Google Scholor - Tian, P., Liu, Y., Li, Z. J., Xu, G. J., & Ma, X. L. (2021). Zoledronic acid in osteoporotic vertebral compression fractures treated with percutaneous kyphoplasty: A meta-analysis. Frontiers in Surgery, 8:668551.
Publisher | Google Scholor - Cecchi, E., Grossi, F., Rossi, M., Giglioli, C., & De Feo, M. L. (2015). Severe hypocalcemia and life-threatening ventricular arrhythmias: Case report and proposal of a diagnostic and therapeutic algorithm. Clinical Cases in Mineral and Bone Metabolism, 12(3):265–268.
Publisher | Google Scholor - Khalid, S., Albaba, I., & Neu, K. (2023). Hypocalcemia: A little-known cause of supraventricular tachyarrhythmia. Cureus, 15(1):e38456.
Publisher | Google Scholor - Vallejo Garcia, V., Gonzalez Calle, D., Castro Garay, J. C., et al. (2021). Functional mitral regurgitation in dilated cardiomyopathy: Clinical implications and prognosis. European Heart Journal – Cardiovascular Imaging, 22(Supplement 3):jeaa356.361.
Publisher | Google Scholor - Dickerman, S. A., & Rubler, S. (1989). Mitral and tricuspid valve regurgitation in dilated cardiomyopathy. The American Journal of Cardiology, 63(8):629–631.
Publisher | Google Scholor - Mangieri, A., Montalto, C., Pagnesi, M., et al. (2017). Mechanisms and implications of tricuspid regurgitation: From the pathophysiology to current and future therapeutic options. Circulation: Cardiovascular Interventions, 10(7):e005043.
Publisher | Google Scholor - Bach, D. S., & Bolling, S. F. (1996). Improvement following correction of secondary mitral regurgitation in end-stage cardiomyopathy with mitral annuloplasty. American Journal of Cardiology, 77(12):966–969.
Publisher | Google Scholor























