

Case Report
Post-Traumatic Aortic Dissection in a Pediatric Patient-Case Report
- Priscila Martins ID 1*
- Mauro Roberto Basso ID 2
- Andrea Morgato de Mello Miyasaki ID 3
- Ricardo Silva Parreira ID 3
- Susy Oliveira de Andrade ID 4
1Resident Physician in Pediatric Surgery - University Hospital - State University of Londrina, Brazil.
2Assistant Professor and Head of the Pediatric Surgery Service - University Hospital - State University of Londrina, Brazil.
3Assistant Professor of the Pediatric Surgery Service - University Hospital - State University of Londrina, Brazil.
4Resident Physician in Pediatric Surgery - University Hospital - State University of Londrina, Brazil.
*Corresponding Author: Priscila Martins, Resident Physician in Pediatric Surgery - University Hospital - State University of Londrina, Brazil.
Citation: Martins P., Basso MR, Miyasaki AMM., Parreira RS, Andrade SO. (2026). Post-Traumatic Aortic Dissection in a Pediatric Patient - Case Report. Journal of Surgical Case Reports and Reviews. BioRes Scientia Publishers. 5(1):1-4. DOI: 10.59657/2993-1126.brs.26.031
Copyright: © 2026 Priscila Martins, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: September 12, 2025 | Accepted: February 25, 2026 | Published: March 04, 2026
Abstract
Post-traumatic aortic dissection in pediatric patients is a rare but potentially fatal condition, usually resulting from high-energy blunt thoracic and abdominal trauma, such as motor vehicle accidents or falls from a great height. In this condition, the layers of the aortic wall separate themselves, forming a false lumen, which can compromise perfusion of specific organs and lead to aortic rupture and its devastating consequences. We report the case of a child who developed a post-traumatic abdominal aortic dissection, which was treated non-operatively and evolved satisfactorily and with good outcome. Although surgical management is traditionally indicated due to the risk of serious complications, conservative treatment has gained favor in selected cases, especially when the dissection is stable and limited, and the patient is in good clinical condition.
Keywords: aortic dissection; pediatrics; thoracoabdominal trauma; traumatic aortic injury
Introduction
Trauma remains the leading cause of death in children, but traumatic vascular injuries, and aortic injuries in particular, are rarely encountered in the pediatric trauma population [1]. Approximately 0.6% of all pediatric trauma patients experience some form of vascular injury [2]. Aortic dissection refers to necrosis or degeneration of the medial layer of the aortic wall [1]. When the intima is damaged or ruptured, blood enters the medial layer and forms a hematoma that extends distally, dissecting the wall layers, causing continuous disruption of the vessel wall [2]. There is a paucity of reports in the literature on pediatric cases, and misdiagnosis is common due to nonspecific symptoms, lack of experience among medical staff, and lack of consensus and guidelines [3].
Case Report
Patient S.C.D.M., a 3-year-old male, was brought by emergency medical transport after a high-speed car rollover. He was admitted hemodynamically stable, on an oxygen mask, with a Glasgow Coma Scale score of 14, opening his eyes upon being called and reporting diffuse abdominal pain. Physical examination revealed a distended abdomen with ecchymosis in the pelvic region consistent with the seat belt sign. After clinical stabilization, he underwent a contrast-enhanced abdominal tomography (CT scan), which identified a normal-sized abdominal aorta with parietal irregularities resembling a dissection flap in the infrarenal segment and at the emergence of the right common iliac artery, suggestive of areas of dissection (Figure 1). There were no signs of intravenous contrast extravasation into the peritoneal cavity. The abdominal aorta measured approximately 5.6 mm before the dissection and 8 mm in the dissected infrarenal region with the false lumen (Figure 2). The lesion was classified as a Stanford type B aortic dissection.
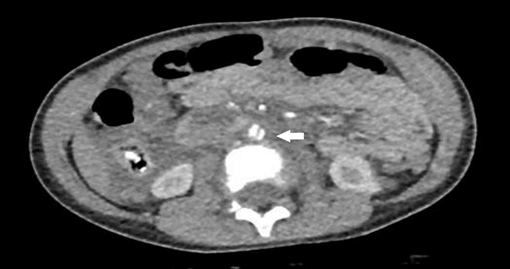
Figure 1: Contrast-enhanced abdominal tomography that identified the abdominal aorta presenting parietal irregularities with a dissection flap appearance in the infrarenal segment (arrow), with no signs of intravenous contrast extravasation into the peritoneal cavity.
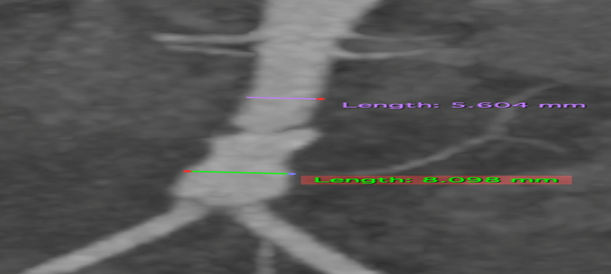
Figure 2: Contrast-enhanced abdominal tomography showing the abdominal aorta measuring approximately 5.6 mm before dissection and 8 mm in the dissected infrarenal region with the false lumen.
Due to clinical and hemodynamic stability, conservative treatment of the dissection was initially chosen, with monitoring in the pediatric intensive care unit (ICU) and serial hemoglobin and hematocrit measurements. Twelve hours after the trauma, the patient developed severe abdominal pain, refractory to opioid analgesia, and worsening abdominal distension.
He underwent exploratory laparotomy, which revealed a large mesenteric hematoma, affecting a small intestine segment measuring approximately 7 cm, with a loop on the verge of perforation. An enterectomy of this segment was performed, resulting in hematoma and end-to-end enteroanastomosis. A non-pulsatile, non-expanding retroperitoneal hematoma was also identified, and conservative management was chosen.
The patient progressed satisfactorily after the procedure, with good dietary compliance, preserved physiological habits, and reporting little or no abdominal pain. On the 10th postoperative day, he underwent abdominal CT angiography to monitor the progression of the aortic dissection. The follow-up images did not reveal the aortic dissection flap seen on the initial CT scan. After 12 days of hospitalization, the patient was discharged for outpatient follow-up.
One year after the trauma, he underwent an outpatient CT scan, which revealed a patent abdominal aorta with a preserved course, no significant stenosis, and a dissection flap in the infrarenal segment of the aorta, associated with an area of focal reduction in caliber and partial thrombosis of the false lumen. The patient remains asymptomatic and is regularly monitored by the Pediatric and Vascular Surgery teams, with conservative management of the aortic lesions.
Discussion
Traumatic injuries remain the most common cause of death in the pediatric population [1]. An estimated 20,000 children die each year from traumatic injuries [3]. Despite the increasing incidence of penetrating trauma, blunt trauma remains the most common mechanism of injury in children, including motor vehicle accidents, falls, and pedestrian injuries [2,3]. In line with the literature, the patient in this report was the victim of a high-energy motor vehicle accident with blunt abdominal trauma.
Although aortic dissection is common in adults, it is a very rare and potentially fatal condition in children, associated with connective tissue disorders, congenital heart disease, and thoracoabdominal trauma [2]. Currently, there are few reported cases of aortic dissection in children under 16 years of age, and relevant statistics are scarce. There is still no consensus among experts regarding the pathophysiology, clinical presentation, and choice of surgical approach [1].
Aortic dissection occurs when blood enters the medial layer of the aortic wall after a rupture or degeneration of the vessel's tunica intima, creating a blood-filled channel within the aortic wall, called a "false lumen," forming a hematoma that extends distally [3].
This dissecting intramural hematoma can rupture into the pericardial, pleural, or peritoneal cavities [2]. The branch arteries of the aorta may become partially or completely occluded. Static obstruction occurs when the dissecting hematoma crosses or completely penetrates the opening of a branch artery. Dynamic obstruction involves complete or partial coverage of the branch artery opening by a flap of dissected aortic wall, without the hematoma dissecting into the branch artery. A combination of dynamic and static obstruction can also occur [3,4].
The onset and spread of most aortic dissections are believed to involve the interaction of genetic factors, inflammatory processes, hypertension, medication use, or lifestyle, as well as certain predisposing conditions that can intrinsically weaken the medial layer of the aortic wall, which is composed of elastin, collagen, and smooth muscle [4].
There are two main classifications for aortic dissection: DeBakey and Stanford. The DeBakey classification is more detailed, describing the origin and extent of the aortic dissection, while the Stanford classification is simpler and more practical, used to define treatment [2,5]. The most common type of aortic dissection is Stanford type B, with the abdominal aorta being the most frequently affected site [1,4]. Consistent with the literature, the patient in this report presented an abdominal lesion classified as Stanford B.
Adult cases are frequently associated with hypertension, hyperlipidemia, and atherosclerosis, while pediatric cases are primarily associated with congenital cardiovascular diseases, inherited connective tissue disorders, and genetic conditions such as Marfan syndrome and Ehlers-Danlos syndrome [4,5].
Aortic injury associated with blunt abdominal trauma is rare and may be present in patients who present with the seat belt sign on physical examination [7]. In 1979, Dajee et al. first described the "seat belt aorta" as a variety of aortic injuries sustained by 2- and 3-point restraint systems, including abdominal aortic dissection and thrombosis [7]. In the case reported here, the seat belt sign was one of the initial physical examination findings.
Physical signs of acute aortic dissection primarily involve the cardiovascular, pulmonary, and neurological systems [5]. Signs of orthostatic hypotension may be present. Shock may be caused by mid-aortic hemorrhage, aortic rupture, pericardial tamponade, or acute heart failure [6].
Cases reported in the literature primarily presented with chest and/or abdominal pain and dyspnea [6]. It is also crucial to understand the mechanism of injury. High-energy trauma is more likely to cause significant injuries, even without a thorough initial physical examination [7]. Therefore, when evaluating pediatric patients with chest and abdominal pain, one should always correlate the findings with the kinematics of the trauma and promptly perform relevant ancillary imaging studies if the symptoms cannot be adequately explained by the patient's history and physical examination [6,7].
Chest and abdominal CT angiography has demonstrated the best sensitivity and specificity in diagnosing aortic dissection, clearly identifying the type, extent of involvement, and even ruptures [8,9]. Echocardiography can also be used as a preliminary screening method in pediatric patients with lesions in the ascending aorta [8].
Treatment options for aortic dissection, as in adults, include open surgical repair, endovascular intervention, or hospital observation with conservative treatment [7]. Currently, there are no specific guidelines for the treatment of aortic dissection in children, and its management relies largely on adult treatment protocols, including pain control, heart rate control, and blood pressure reduction [8,9].
Treatment of this condition depends on the lesion classification system, whether DeBakey or Stanford, and the patient's clinical condition [10]. Timely surgical intervention will be necessary when the lesion classification and the patient's clinical status dictate. Surgical approaches, including aortic replacement, endovascular repair, and covered stent implantation, should be selected based on the clinical classification of pediatric patients [8,9].
Non-operative treatment is based on continuous monitoring of the aortic lesion and the patient's clinical condition. It involves strict control of blood pressure and heart rate, usually with beta-blockers, as well as hemodynamic and imaging monitoring, such as CT angiography [9,10]. Ultrasonography is advantageous due to the absence of radiation exposure and its ability to demonstrate turbulent flow, if present. Furthermore, using the same imaging technique in subsequent examinations will simplify comparisons between studies [10].
Conclusion
In pediatrics, the decision for non-operative management requires careful multidisciplinary evaluation, considering surgical risks, lesion pattern, and clinical response to drug therapy. Limited evidence suggests that, in well-selected cases, conservative treatment can be effective, safe, and less invasive, avoiding surgery-related complications. Given the rarity of aortic dissection in children, and therefore the scarcity of studies in the literature, individualized treatment and rigorous long-term follow-up are essential.
Conflict of Interest
No.
References
-
-->




















