

Case Report
Ocular Ischemic Syndrome: A Rare Bilateral Presentation in a Hypertensive Patient-A Case Report
1Assistant Professor, Department of Optometry, Royal Global University, Assam, India.
2Consultant Optometrist, Mobile Medical Unit, Assam, India.
*Corresponding Author: Haziel Rynjah, Assistant Professor, Department of Optometry, Royal Global University, Assam, India.
Citation: Rynjah H, Choudhury NA. (2025). Ocular Ischemic Syndrome: A Rare Bilateral Presentation in a Hypertensive Patient - A Case Report, International Journal of Biomedical and Clinical Research, BioRes Scientia Publishers. 4(5):1-3. DOI: 10.59657/2997-6103.brs.25.100
Copyright: © 2025 Haziel Rynjah, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: October 09, 2025 | Accepted: November 14, 2025 | Published: November 20, 2025
Abstract
Background: Ocular Ischemic Syndrome (OIS) is a rare, vision-threatening disorder resulting from chronic hypoperfusion of the ocular tissues due to carotid artery occlusive disease. It may present with a combination of anterior and posterior segment ischemic changes and often reflects underlying systemic vascular compromise.
Case Presentation: A 59-year-old male with a two-year history of hypertension presented with gradual blurring of vision in both eyes for three years. No history of ocular trauma or prior eye disease was reported. Ocular examination revealed best-corrected visual acuity (BCVA) of 6/24 in both eyes with compound hyperopic astigmatism and presbyopia. Slit-lamp and fundus evaluation showed retinal hemorrhages and cotton-wool spots bilaterally, suggestive of ocular ischemic changes. Intraocular pressures were within normal limits. Optical Coherence Tomography (OCT) of the macula revealed ischemic retinal changes.
Management: The patient received intravitreal anti-VEGF (Avastin) injections in both eyes, followed by panretinal photocoagulation (PRP) after the first injection. Systemic evaluation for carotid artery stenosis and cardiovascular risk factors was advised in collaboration with a neurologist and a physician.
Conclusion: Early recognition of OIS is crucial as it may be the first clinical manifestation of severe carotid artery disease. Timely ophthalmic and systemic interventions can prevent irreversible visual loss and life-threatening cerebrovascular events.
Keywords: ocular ischemic syndrome; carotid artery stenosis; anti-VEGF; panretinal photocoagulation; retinal ischemia
Introduction
Ocular Ischemic Syndrome (OIS) is a vision-threatening condition characterized by ocular hypoperfusion secondary to severe carotid artery obstruction. It manifests acutely as amaurosis fugax or central retinal artery occlusion and chronically as ischemic retinopathy and neovascular glaucoma [1]. Approximately 80% of OIS cases exhibit gradual vision loss, whereas a smaller subset presents with sudden visual decline due to neovascular complications [2]. OIS is typically associated with ipsilateral internal carotid artery (ICA) stenosis, leading to an estimated 50% reduction in central retinal artery perfusion pressure [3]. Given its association with systemic vascular disorders such as hypertension, diabetes, and coronary artery disease, prompt detection and interdisciplinary management are vital.
Case Presentation
Patient Information: A 59-year-old male presented to the eye clinic with complaints of gradual blurring of vision for both distance and near over the past three years. There was no history of ocular trauma or prior eye conditions.
Medical History: The patient was known hypertensive for two years and was on regular antihypertensive medication. No history of diabetes, cardiovascular disease, or cerebrovascular events was reported.
Family and Allergy History: No significant family ocular history or known allergies.
Ocular Examination
| Parameter | Right Eye (OD) | Left Eye (OS) |
| Visual Acuity (Unaided) | 6/36 | 6/60 |
| Pinhole | 6/24 | 6/24 |
| Near Vision | N36 @40 cm | N36 @40 cm |
| Objective Refraction | +1.25 / +1.00 × 180° | +1.50 / +1.00 × 180° |
| BCVA | +1.00 / +1.00 × 180° 6/24 | +1.00 / +1.00 × 180° 6/24 |
| Add | +2.75 N12 | +2.75 N18 |
| Intraocular Pressure (AT @9:14am) | 12 mmHg | 12 mmHg |
Ocular Alignment: Orthophoria at distance and near.
Ocular Motility: Full in both eyes.
External Examination: Normal facial symmetry, head posture, and adnexa.
Slit-Lamp and Fundus Examination
| Findings | Right Eye (OD) | Left Eye (OS) |
| Eyelids & Adnexa | Normal | Normal |
| Conjunctiva | Clear | Clear |
| Cornea | Clear | Clear |
| Anterior Chamber | Normal depth | Normal depth |
| Lens | Clear | Clear |
| Iris | Normal | Normal |
| Pupil Reaction | RRR | RRR |
| Vitreous | Clear | Clear |
| Fundus (Dilated Exam) | C/D 0.3, NRR Healthy, Retinal hemorrhages, Cotton-wool spots | C/D 0.3, NRR Healthy, Retinal hemorrhages, Cotton-wool spots |
| Retinal Periphery | Normal | Normal |
OCT Macula (Both Eyes): Evidence of ischemic retinal changes consistent with OIS.
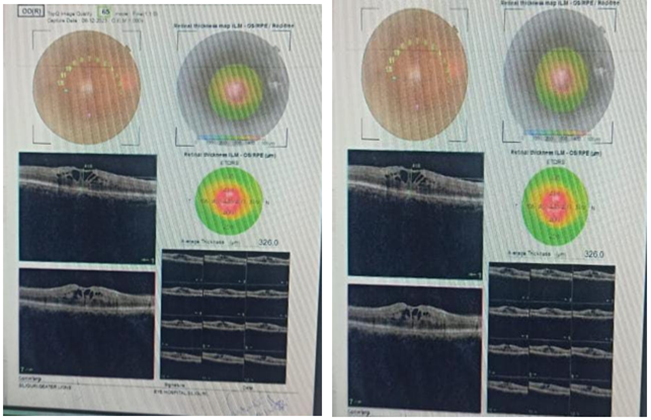
Figure 1: OCT report of OIS in BE.
Diagnosis
- Ocular Ischemic Syndrome (Bilateral).
- Compound Hyperopic Astigmatism (Both Eyes).
- Presbyopia (Both Eyes).
Management and Follow-Up
Ocular Treatment
- Intravitreal Bevacizumab (Avastin) injection in both eyes.
- Panretinal Photocoagulation (PRP) after the first anti-VEGF injection to reduce ischemia-induced neovascularization.
- Avoidance of intraocular pressure-raising agents (e.g., prostaglandin analogues, pilocarpine).
Systemic Evaluation
- Referred for carotid Doppler ultrasonography and cardiovascular assessment.
- Blood pressure monitoring and optimization of antihypertensive therapy.
Surgical Consideration
- No immediate surgical indication, as neovascularization and neovascular glaucoma were not yet present.
Discussion
Ocular Ischemic Syndrome is often underdiagnosed due to its variable presentation and overlap with diabetic or hypertensive retinopathy. It typically develops secondary to severe (>90%) ipsilateral carotid artery stenosis, resulting in reduced ocular perfusion [2,3]. The patient presented here had hypertension, a known vascular risk factor for carotid disease, highlighting the systemic connection between ocular and cerebrovascular pathology [4,5]. Studies by Mendrinos et al. (2010) and Ishii et al. (2016) emphasize the importance of correlating ophthalmic findings with carotid Doppler imaging and systemic vascular work-up. In this case, prompt anti-VEGF and PRP therapy were initiated to prevent neovascular complications, with concurrent systemic evaluation to address underlying vascular insufficiency.
Conclusion
Ocular Ischemic Syndrome signifies not only a threat to vision but also a potential harbinger of life-threatening cerebrovascular disease [6]. Early ophthalmic detection, coupled with systemic management of vascular risk factors, is vital for preserving vision and preventing morbidity. The prognosis depends on the stage at diagnosis. Early intervention before the onset of neovascular glaucoma offers the best outcome.
References
- Ishii, M., Hayashi, M., Yagi, F., Sato, K., Tomita, G., et al. (2016). Relationship between the direction of ophthalmic artery blood flow and ocular microcirculation before and after carotid artery stenting. Journal of Ophthalmology, 1:2530914.
Publisher | Google Scholor - Ganaie, H. A., Gupta, V., Parthasarathy, R., Londhe, S., Anand, S. (2020). Blindness following carotid artery stenting due to ocular hyperperfusion-report and review of literature. Neurology India, 68(4):897-899.
Publisher | Google Scholor - Hussain, N., Jalali, S., Kaul, S. (2001). Carotid artery disease and ocular vascular disorders. Indian Journal of Ophthalmology, 49(1):5-14.
Publisher | Google Scholor - Mendrinos, E., Machinis, T. G., Pournaras, C. J. (2010). Ocular ischemic syndrome. Survey of Ophthalmology, 55(1):2-34.
Publisher | Google Scholor - Hedges Jr, T. R. (1963). Ophthalmoscopic findings in internal carotid artery occlusion. American Journal of Ophthalmology, 55(5):1007-1012.
Publisher | Google Scholor - Wang, H., Li, H., Zhang, X., Qiu, L., Wang, Z., et al. (2017). Ocular image and haemodynamic features associated with different gradings of ipsilateral internal carotid artery stenosis. Journal of Ophthalmology, 1:1842176.
Publisher | Google Scholor























