

Research Article
Obesity and Lifestyle: An Assessment of Social and Psychological Factors Based on 1031 Patients
- Serpil Sevimli Deniz ID 1*
- Nevra Karademir ID 2
- İbrahim Doğan ID 3
- Mehmet Kadir Bartın ID 4
- Ezgi Sönmez ID 5
- Remzi Sarıkaya ID 6
- Sebahattin Çelik ID 7
1 Van Yüzüncü Yıl University, Van, Türkiye.
2 University of Health Sciences, Van Training and Research Hospital, Türkiye.
3 University of Health Sciences, Van Training and Research Hospital, Department of Internal Medicine, Türkiye.
4 University of Health Sciences, Van Training and Research Hospital, Türkiye.
5 University of Health Sciences, Van Training and Research Hospital, Department of Internal Medicine, Türkiye.
6 University of Health Sciences, Van Training and Research Hospital, Department of Cardiology, Türkiye.
7 University of Health Sciences, Van Training and Research Hospital, Türkiye.
*Corresponding Author: Serpil Sevimli Deniz, Van Yüzüncü Yıl University, Van, Türkiye.
Citation: Serpil S. Deniz, Karademir N, Doğan I, Mehmet K. Bartın, Sönmez E, et al. (2025). Obesity and Lifestyle: An Assessment of Social and Psychological Factors Based on 1031 Patients, Clinical Case Reports and Studies, BioRes Scientia Publishers. 10(3):1-6. DOI: 10.59657/2837-2565.brs.25.263
Copyright: © 2025 Serpil Sevimli Deniz, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: June 18, 2025 | Accepted: July 02, 2025 | Published: July 09, 2025
Abstract
Objective: This study was conducted to determine the effects of eating habits, physical activity levels, body image perceptions, and mental states on obesity management among individuals registered at an obesity center. The study examined the relationships between these factors and their contributions to success in weight control.
Methods: The study was conducted with a prospective design between 2019 and 2024. A total of 1031 individuals with a body mass index (BMI) of 30 or above were included in the study. Participants completed demographic information forms, the Beck Depression Inventory, the Body Image Scale, and tools for assessing physical activity and nutrition. The data were analyzed using ANOVA, correlation, Chi-square, and t-tests.
Results: A total of 1031 individuals participated in the study, including 922 women and 109 men. Among the participants, 801 were married, and 221 were single. The mean age was 40.82±12.29 years, and the mean BMI was 39.44±6.02. Significant differences were found among obesity groups (BMI: 30-35, 35-40, >40) in terms of physical activity, eating habits, and mental state. In the BMI 30-35 group, the use of extra fat was significantly different compared to other groups (p < 0.05). While no significant differences in depression scores were observed among obesity groups, a positive correlation was identified between body image and depression scores (p < 0.05). Physical activity levels significantly differed across BMI categories (χ² = 62.14, p = 0.0000317), and the frequency of eating at restaurants was found to impact weight control (χ² = 52.10, p = 0.00076). Furthermore, a significant difference in depression scores was identified between male and female participants.
Conclusion: This study revealed significant differences among obesity groups in terms of physical activity, eating habits, and mental state. In particular, the significant difference in the use of extra fat among individuals in the BMI 30-35 group compared to other groups highlights the critical role of eating habits in obesity management. Physical activity levels were found to vary across BMI categories, and the habit of eating at restaurants was identified as influencing weight control. Furthermore, the positive relationship observed between body image and depression underscores the impact of individuals' mental states on obesity management. The difference in depression scores between male and female participants points to the influence of gender on mental health. These findings suggest that personalized approaches may enhance the effectiveness of obesity treatment.
Keywords: obesity; body mass index; eating habits; lifestyle; behavioral style
Introduction
Obesity is defined by the World Health Organization (WHO) as abnormal or excessive fat accumulation that may impair health. It is commonly assessed using the Body Mass Index (BMI), which is calculated by dividing a person’s weight in kilograms by the square of their height in meters. According to WHO classifications, a BMI below 18.5 is considered underweight. Values between 18.5 and 24.9 are categorized as normal weight. A BMI between 25.0 and 29.9 indicates overweight, while a BMI of 30.0 and above is classified as obese. Specifically, a BMI between 30.0 and 34.9 is referred to as Class I obesity (mild obesity), 35.0 to 39.9 as Class II obesity (moderate obesity), and 40.0 or above as Class III obesity (morbid obesity).
Obesity is a rapidly growing health concern in both developed and developing countries, with serious consequences for individual and public health. Its effects extend beyond physical health issues, also negatively impacting individuals' social and psychological well-being. This study aims to address the knowledge gap in this area by evaluating the influence of lifestyle variables as well as social and psychological factors on obesity. Specifically, the study investigates how lifestyle characteristics such as social behaviors, eating habits, physical activity levels, and mental health status affect obesity management among individuals registered at an obesity center.
The research examines differences in physical activity, dietary habits, and psychological states across various BMI groups. Additionally, it explores the relationship between positive body image and depression levels. The association between daily physical activity and weight control is analyzed to assess its effect on successful weight management. The impact of the frequency of eating out at restaurants on weight control success is also evaluated. Finally, potential differences in depression scores between male and female participants are analyzed.
Method
This research was designed as a descriptive and correlational study. Within the scope of the study, lifestyle variables such as social behaviors, eating habits, physical activity levels, and psychological status of individuals registered at an obesity center were evaluated from a long-term perspective.
Study Setting and Period
The study was conducted with individuals registered at a “Tertiary Education and Research Hospital Obesity Center” established in full accordance with the regulations created under the framework of the obesity prevention policy of the Turkish Ministry of Health. The research was carried out prospectively between the years 2019 and 2024.
Population and Sample
Population: The study population consisted of individuals registered at an obesity center who regularly attended follow-ups.
Sample: The study sample included 1,031 individuals who were regularly followed between 2019 and 2024. Inclusion criteria were as follows: individuals with a Body Mass Index (BMI) of 30 or above, at least one year of regular follow-up history, complete and accurate records of social, behavioral, and psychological data, and provision of informed consent.
Exclusion criteria included individuals receiving regular psychiatric treatment, those with incomplete or inaccurate data, pregnant or breastfeeding women, and individuals who did not participate regularly in follow-up visits during the study period.
Data Collection Tools
To evaluate the participants' social behaviors, eating habits, physical activity levels, and psychological status, the following data collection tools were used:
Personal Information Form
Developed to collect participants’ demographic information (age, gender, marital status) and medical history (BMI, current health status).
Beck Depression Inventory-II (BDI-II)
Used to assess participants’ level of depression. The Turkish version of this scale was validated for reliability and validity by Kapci et al. (2008), and found to be a reliable tool.
Body Image Scale (BIS)
Used to assess participants’ body image perception. The Turkish adaptation’s reliability and validity were confirmed by Karayurt et al. (2015).
Physical Activity Assessment Form
Designed to determine the participants' level of physical activity. Weekly walking habits, participation in sports, and general daily mobility levels were recorded.
Eating Habits Assessment Form
Created to evaluate eating habits such as frequency of eating out at restaurants, eating before bed, and extra fat consumption.
Data Collection Method
The personal information form and scales were administered to the participants during face-to-face interviews. Body weight and height measurements were taken, and Body Mass Index (BMI) was calculated accordingly. Social and behavioral data were recorded through structured forms.
The flowchart below illustrates the participant selection process and their distribution according to BMI categories.
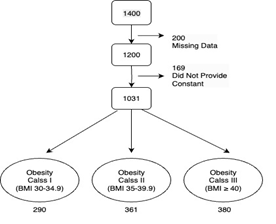
Figure 1: Selection Process and BMI Category Distribution of Participants
Data Analysis
The data were analyzed using the SPSS 25.0 statistical software package. To assess the relationships between the variables and obesity, ANOVA, correlation analysis, chi-square test, and t-test were used. A p-value of less than 0.05 was considered statistically significant in all analyses.
Results
The study included a total of 1,031 participants, comprising 922 women and 109 men. Among them, 801 were married and 221 were single.
Table 1: Characteristics of the Participants (n = 1031)
| Variables | Mean ± SD |
| Age (range: 17–75) | 40.82 ± 12.29 |
| Initial Weight (kg) | 103.44 ± 17.25 |
| Height (m) | 1.61 ± 0.07 |
| Body Mass Index (BMI) | 39.44 ± 6.02 |
| Nutrition Habits - Physical Activity Score* | 5.35 ± 0.95 |
| Nutrition Habits - Extra Fat Usage Score* | 3.3 ± 1.13 |
| Beck Depression Inventory (BDI) | 13.78 ± 8.1 |
| Body Image Perception - General Score* | 1.58 ± 0.69 |
* Since the data were not normally distributed, median ± standard deviation values were reported.
Table 2: Summary of Depression, Physical Activity, Extra Fat Use, Restaurant Eating Frequency, and Body Image Scores by BMI Categories.
| Variable | BMI 30–34.9 | BMI 35–39.9 | BMI ≥ 40 |
| Depression Scores (Mean ± SD) | 14.22 ± 8.05 | 13.8 ± 8.97 | 13.54 ± 7.31 |
| Physical Activity Levels (Mean ± SD) | 5.64 ± 0.73 | 5.38 ± 0.95 | 5.17 ± 1.0 |
| Extra Fat Use (Mean ± SD) | 3.41 ± 1.08 | 3.39 ± 1.06 | 3.15 ± 1.19 |
| Restaurant Eating Frequency (Mean ± SD) | 4.24 ± 1.30 | 4.25 ± 1.31 | 4.35 ± 1.30 |
| Body Image Scores (Mean ± SD) | 1.43 ± 0.70 | 1.54 ± 0.74 | 1.67 ± 0.63 |
In the dataset, there were 290 individuals in the Obesity Class I (BMI 30–34.9), 361 in Obesity Class II (BMI 35–39.9), and 380 in Obesity Class III (BMI ≥ 40). Statistical analyses among these categories revealed significant differences in terms of physical activity, nutritional habits, and psychological status.
Post-hoc analyses showed that individuals in the BMI 30–34.9 group differed significantly from other obesity groups in terms of extra fat consumption (p less than 0.05). Although there was no statistically significant difference in depression scores among the obesity categories, a moderate positive correlation was found between body image perception scores and depression levels (p less than 0.05). This finding suggests that negative body image may influence the level of depression in individuals.
It was observed that physical activity levels differed significantly across BMI categories (χ² = 62.14, p = 0.0000317), indicating that physical activity is a contributing factor to BMI. Similarly, a statistically significant relationship was found between the frequency of eating at restaurants and BMI categories (χ² = 52.10, p = 0.00076), suggesting that frequent restaurant meals may impact weight control.
Lastly, a statistically significant difference was found between men and women in terms of depression scores (p less than 0.05).
Discussion
In the literature, it is frequently emphasized that obesity has significant effects on individuals both physically and psychosocially (Andrei et al., 2018). The findings of our study revealed that female participants had significantly higher depression scores compared to males, which appears to be associated with social pressure and body image perception. This finding is supported by previous studies (İpek, 2019; Kılıç, 2020; Mermi, 2018), which highlight that women carry a greater psychosocial burden related to obesity, contributing to depression and low self-esteem. The higher depression scores among women point to the gender-specific impact of obesity.
Stunkard and Wadden (1992) stated that individuals with obesity are more likely to experience depression, which is linked to distorted body image. Rand et al. (2017) noted that psychological and social well-being are critical factors influencing weight control. Similarly, Sagar and Gupta (2018) found that psychological issues caused by obesity, particularly in children and adolescents, may have lifelong consequences. In alignment with these findings, our study demonstrates the impact of women's body image perception on depression and weight control.
Participants with lower BMI were found to have higher levels of physical activity, supporting the findings of Wing and Hill (2001) and Lavie et al. (2015), who emphasized the critical role of regular physical activity in weight control and overall health. Wing and Hill (2001) emphasized that maintaining regular physical activity is essential for sustainable weight loss, while Lavie et al. (2015) noted that physical activity contributes not only to weight management but also to cardiovascular health. Our study underscores the importance of implementing community-based programs to promote physical activity for effective weight management.
The higher frequency of restaurant eating among participants in higher BMI groups is consistent with Lavie et al.'s (2015) findings that restaurant meals are generally high in calories and low in nutritional value. Furthermore, increased extra fat consumption was more common among those with higher BMI. Fuentes et al. (2019) highlighted that socioeconomic factors can trigger unhealthy eating habits, thereby increasing the risk of obesity. Our study confirms that frequent restaurant meals and unhealthy dietary habits are major barriers to successful weight management.
The impact of socioeconomic status on obesity management was clearly observed in our findings. Individuals with lower socioeconomic status were found to have unhealthier eating habits and lower physical activity levels. These results are consistent with the findings of Beyaz (2020) and the World Health Organization (2016), which report that low-income groups are more exposed to unhealthy foods and have limited access to opportunities for physical activity. Yumuk et al. (2015) emphasized that socioeconomic status directly affects individuals' ability to cope with obesity, highlighting the importance of social policies.
It is evident that factors such as depression, physical activity, and eating habits are interrelated in obesity management. Calugi and Dalle Grave (2020) investigated the role of psychological factors in obesity and reported that emotional eating behaviors pose a major barrier to weight control. Stunkard and Wadden (1992) emphasized the importance of addressing not only the physical but also the psychological aspects of severe obesity. These findings indicate the critical importance of incorporating psychosocial approaches and emotional support in obesity treatment.
Observations of psychological improvement following surgical interventions further demonstrate the necessity of a holistic treatment approach. Kökönyei (2020) also emphasized that emotional regulation strategies such as emotional eating and rumination are strongly associated with obesity. Our study supports these findings by highlighting the influence of depression and psychosocial factors on weight control.
Conclusion and Recommendations
This study revealed significant differences among obesity groups in terms of physical activity, eating habits, and psychological status. In particular, the distinction observed in extra fat consumption among individuals in the BMI 30–35 group highlights the critical role of dietary habits in obesity management. Physical activity levels significantly varied by BMI categories, and the frequency of eating out was found to affect weight control. Furthermore, a positive correlation was identified between body image perception and depression scores, indicating the impact of psychological well-being on obesity management. The statistically significant differences in depression scores between male and female participants underline the gender-specific psychological effects of obesity.
These findings emphasize the importance of psychological, social, and behavioral factors in obesity treatment.
Recommendations
Promoting Physical Activity: Community-based physical activity programs should be prioritized to support weight control and general health.
Improving Dietary Habits: Health education programs should aim to reduce unhealthy eating behaviors, such as excessive fat consumption and frequent restaurant meals.
Psychosocial Support Services: Support programs addressing body image and mental health concerns, such as depression, should be incorporated into obesity management.
Gender-Specific Interventions: Intervention strategies should be designed to address the unique needs of both men and women.
Personalized Treatment Plans: Obesity management strategies should be tailored to individual needs to enhance treatment effectiveness.
These results indicate that obesity should be addressed as a biopsychosocial issue and that multidimensional approaches can improve not only weight control but also overall well-being. Comprehensive and sustainable strategies will offer effective solutions in combating obesity.
Limitations of the Study
Sample Constraints: The study was limited to a specific region, reducing generalizability.
Self-Reported Data: The use of self-reported questionnaires may pose a risk of bias and error.
Cross-Sectional Design: Causal relationships cannot be inferred due to the study's cross-sectional nature.
Limited Analysis of Psychosocial Factors: Other relevant variables such as stress and anxiety were not analyzed in detail.
Demographic Imbalance: A large proportion of participants (89.43%) were female.
Lack of Longitudinal Data: Changes over time could not be monitored.
Lack of Objective Measurements: Variables such as physical activity were not measured using objective tools.
Socioeconomic and Cultural Factors: These variables were not analyzed in depth.
References
- Andrei, F., Nuccitelli, C., Mancini, G., Reggiani, G., & Trombini, E. (2018). Emotional intelligence, emotion regulation and affectivity in adults seeking treatment for obesity. PsychiatryResearch, 269:191-198.
Publisher | Google Scholor - Beyaz, Z. (2020). Türkiye’de obezite üzerine sosyoekonomik faktörlerin etkisi ve gelir eşitsizliği. Academia. Erişim adresi.
Publisher | Google Scholor - Calugi, S., & DalleGrave, R. (2020). Psychologicalf eatures in obesity: A network analysis. The International Journal of EatingDisorders.
Publisher | Google Scholor - Dünya Sağlık Örgütü. (2016). Global obesity report: Socio economic disparities and risk factors. World Health Organization Reports.
Publisher | Google Scholor - Fuentes, S., Brondeel, R., Franco, M., Sureda, X., Traissac, P., et al. (2019). Psycho-social factors related to obesity and their associations with socio economic characteristics: The RECORD study. Eating and Weight Disorders - Studies on Anorexia.
Publisher | Google Scholor - İpek, E. (2019). Türkiye’de Obezitenin Sosyoekonomik Belirleyicileri. Uluslararası İktisadi Ve İdari İncelemeler Dergisi(25):57-70.
Publisher | Google Scholor - Kapçi, E. G., Uslu, R., Türkapar, H., & Karaoğlan, A. (2008). Beck Depression Inventory II: Evaluation of the psychometric properties and cut‐off points in a Turkish adult population. Depressionand Anxiety, 25.
Publisher | Google Scholor - Karayurt, Ö., Edeer, A. D., Süler, G., Dorum, H., Harputlu, D., Vural, F., & Üçer, C. (2015). Psychometric Properties of the Body Image Scale in Turkish Ostomy Patients. International Journal of Nursing Knowledge, 26(3):127-134.
Publisher | Google Scholor - Kılıç, S. (2020). Duygusal yeme ve obezite arasındaki ilişki: Duygu düzenleme stratejilerinin rolü. FSM Tıp Dergisi, 10(2):112-121
Publisher | Google Scholor - Kökönyei, G., Baldacchino, A., Urbán, R., &Demetrovics, Z. (2020). The psychological basis of obesity. ObesityandObstetrics.
Publisher | Google Scholor - Lavie, C. J., McAuley, P. A., Church, T. S., Milani, R. V., & Blair, S. N. (2015). Obesity and cardiovascular diseases: Implications regarding fitness, fatness, and severity in the obesity paradox. Journal of the American College of Cardiology, 63(14):1345-1354.
Publisher | Google Scholor - Mermi, E. (2018). Obezite ve psikiyatrik hastalıklar arasındaki ilişki: Klinik bir değerlendirme. Fırat Tıp Dergisi, 23(1):45-53.
Publisher | Google Scholor - Rand, K., Vallis, M., Aston, M., Price, S., Piccinini-Vallis, H., Rehman, L., & Kirk, S. (2017). It is not thediet; it is the mental part weneed help with. A multilevel analysis of psychological, emotional, and social well-being in obesity. International Journal of QualitativeStudies on Healthand Well-being, 12.
Publisher | Google Scholor - Sagar, R., & Gupta, T. (2018). Psychological aspects of obesity in children and adolescents. The Indian Journal of Pediatrics, 85:554-559.
Publisher | Google Scholor - Stunkard, A. J., &Wadden, T. A. (1992). Psychological aspects of severe obesity. American Journal of Clinical Nutrition, 55(2):524-532.
Publisher | Google Scholor - Wing, R. R., & Hill, J. O. (2001). Successful weight loss maintenance. Annual Review of Nutrition, 21(1):323-341.
Publisher | Google Scholor - Yumuk, V., Tsigos, C., Fried, M., Schindler, K., Busetto, L., Micić, D., & Toplak, H. (2015). European guidelines for obesity management in adults. ObesityFacts, 8:402-424.
Publisher | Google Scholor























