

Review Article
Modifiable Risk Factors and Cancer Risk: A Systematic Review
1PGY-1 in Neurology, Civil Hospital Larkana, Larkana, Pakistan.
2Medical Student, Chandka Medical College, Larkana, Pakistan.
3PGY 2 in Medicine, Civil Hospital Larkana, Larkana, Pakistan.
4PGY-1 in Hematology, LUMHS hospital, Jamshoro, Pakistan.
5Medical Student, Sir Syed Collage, Karachi, Pakistan.
*Corresponding Author: Parisa Bashir, PGY-1 in Hematology, LUMHS hospital, Jamshoro, Pakistan.
Citation: Rohail A, Tunio J, Hakro A, Ahsan M, Bashir P, et al. (2025). Modifiable Risk Factors and Cancer Risk: A Systematic Review, Journal of Clinical Research and Clinical Trials, BioRes Scientia Publishers. 4(4):1-6. DOI: 10.59657/2837-7184.brs.25.061
Copyright: © 2025 Parisa Bashir, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: July 14, 2025 | Accepted: August 08, 2025 | Published: August 14, 2025
Abstract
Background: Modifiable risk factors for many malignancies can be addressed by modifying one's lifestyle. These include factors like drinking alcohol, smoking cigarettes and being overweight. Physical inactivity, excessive exposure to ultraviolet (UV) radiation, and infections i-e. H.pylori, HBV AND HCV, HIV, HPV and others are additional important risk factors.
Method: Using the electronic databases Google Scholar and PubMed, a comprehensive systematic literature search was conducted between 2010 and 2024. Articles and abstracts published in English were searched. Articles addressing modifiable cancer risk factors and their association with cancer were included. In the meta-analysis, 11 studies met the inclusion criteria after screening the initial set of retrieved articles. Data from these studies were extracted and synthesized to evaluate the association between modifiable risk factors and cancer outcomes.
Results: Percentage of population attributable to various modifiable risk factors related to cancer. Smoking is responsible for the highest PAF at 23.73%, followed by infections at 12.27%. Physical inactivity and obesity contribute moderately at 7.35% and 3.73%, respectively. UV radiation contributes 5.21%, while alcohol intake contributes 4.87%. The results show that modifiable risk factors significantly affect cancer incidence and that lifestyle adjustments may prevent cancer.
Conclusion: There is substantial evidence linking the development of cancer to modifiable risk factors. The incidence of cancer can be considerably decreased by addressing these risk factors and embracing healthy lifestyle choices. This emphasizes how crucial lifestyle changes and preventative actions are to the fight against cancer.
Keywords: cancer; modifiable; smoking; alcohol; infections; UV radiation
Introduction
More than a century ago, Stephen Paget proposed the idea that interactions between cancer cells and their surroundings control the course of the disease [1]. The second most common cause of death globally is cancer. Overall, cancer has become more common; in the United States alone, by 2014, there were over 1,665,540 cancer patients, and 585,720 of them had lost their lives to the disease [2]. With a GDP of US$263 billion and a population of around 220 million, Pakistan is a lower middle-income nation in South Asia as of 2020. Cancer registration needs to be a prerequisite for program planning and assessment in order to reduce the disease's morbidity and death in such a densely populated nation. Actually, it's not so [3]. A study in Pakistan discovered that breast cancer is more common in women and head and neck cancer is more common in men. This is mainly because men consume a lot of harmful substances including cigarettes, betel nut, mainpuri, and gutka [4]. Cancer mortality has decreased as a result of major advancements in early detection, treatment and prevention during the past few decades, as well as in our understanding of the etiology of cancer [5].
Numerous malignancies have a causal relationship with risk factors that may be changed. These risk factors include smoking cigarettes, being overweight, drinking alcohol, eating red and processed meat, not eating enough fruits and vegetables, consuming little fiber, and not getting enough calcium from food, being physically inactive, being exposed to ultraviolet (UV) radiation, and having Helicobacter pylori, hepatitis B virus (HBV), hepatitis C virus (HCV), human herpes virus type 8 (HHV8), HIV, or human papillomavirus (HPV) infections. Removing these risk factors can reverse damage [6,7]. The colon and rectum, prostate, lung and bronchus and bladder have the largest percentages of cancer types in men. The breast, lung and bronchus, colon and rectum, uterine corpus and thyroid are the areas in women where cancer is most common. Blood cancer, brain cancer and lymph node cancer are the three cancer kinds that affect youngsters the most frequently [2].
Objectives
This recent research has shown an increasing correlation between the human cancer burden and the number of modifiable risk factors. Given the continued importance of lifestyle factors like food, physical inactivity, smoking and alcohol use in the development of cancer, a focus on these modifiable hazards has become essential to comprehending cancer trends. Preventive interventions are crucial since research indicates that addressing these factors could result in a significant decrease in cancer incidence and mortality. Scientists are trying to find practical ways to lower cancer rates and enhance public health outcomes by looking at the effects of these risk factors.
Methods
Method: From 2010 to 2024, a comprehensive systematic literature search was conducted utilizing the electronic databases of PubMed and Google Scholar, which contained articles and abstracts written in English. The following keywords were used to search the published abstracts and articles using the aforementioned search engines: "modifiable risk factor," "cancer patients," "smoking," "alcohol intake," "physical inactivity," "Obesity," "infections," "UV radiation," "risk factors in cancer," and "attributable risk factor."
Inclusion Criteria
Following were the study's inclusion criteria:
- Research published from 2010 until 2024.
- Articles discussing the relationship between cancer incidence and modifiable cancer risk factors.
- Modifiable risk factors include alcohol consumption, smoking, infections, physical inactivity, obesity, and UV radiation.
- PAF-based studies. The term "population attributable fraction" (PAF) in cancer refers to environmental or lifestyle variables that raise the risk of cancer and can be changed to lower the overall cancer burden in a community. These include habits that, if altered, could reduce the population's cancer incidence, such as smoking, eating poorly, not exercising, and drinking alcohol. PAF calculates the percentage of cancer cases that could be avoided if certain modifiable risk factors were removed.
- Studies were drawn from different countries, and a total of 11 studies that satisfied the aforementioned inclusion requirements were included.
Exclusion Criteria
Following were the stusy’s exclusion criteria
- Articles that used a non-modifiable risk factor in their studies.
- Article that did not use PAF were not included in this review.
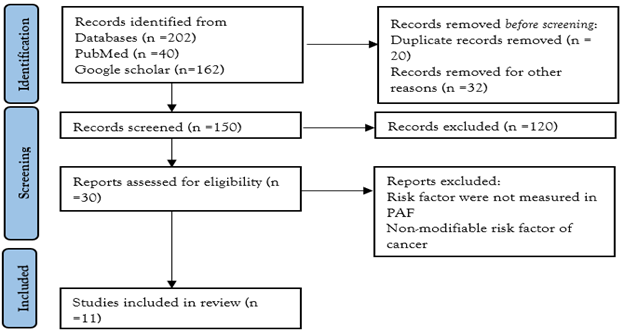
Figure1: PRISMA flow diagram.
Results
Table 1: General Characteristics of The Studies.
| S. No. | Author (Reference) | Year | Country of origin |
| 1 | Islami F (6) | 2018 | United states |
| 2 | Parkin DM (8) | 2011 | United Kingdom |
| 3 | Weiderpass E (9) | 2010 | Norway |
| 4 | Brown KF (10) | 2018 | United Kingdom |
| 5 | Grundy A (11) | 2017 | Canada |
| 6 | Whiteman DC (12) | 2015 | Australia |
| 7 | Collatuzzo G (13) | 2023 | France |
| 8 | Wang JB (14) | 2012 | China |
| 9 | Teh HS (15) | 2021 | Malaysia |
| 10 | Charafeddine MA (16) | 2017 | Lebanon, USA |
| 11 | Poirier AE (17) | 2019 | Canada |
Table 1 shows the basic characteristics of studies included in the meta-analysis.
Table 2: Modifiable Risk Factor (PAF %) Of the Cancer of The Studies.
| References | Smoking (%) | Alcohol (%) | BMI/Obesity (%) | Physical inactivity (%) | Ultraviolent radiation (%) | Infections (%) |
| Islami F, 2018 | 45.5 | 5.6 | 7.8 | 2.9 | 4.7 | 3.3 |
| Parkin DM, 2011 | 19.4 | 4.0 | 5.5 | 1.0 | 3.5 | 3.1 |
| Weiderpass E, 2010 | 18 | 5 | 7 | 2 | N/A | 4 |
| Brown KF, 2018 | 15.1 | 3.3 | 6.3 | 0.5 | 3.8 | 3.6 |
| Grundy A, 2017 | 45.95 | 8.65 | 17.03 | 18.07 | 16.7 | 22.6 |
| Whiteman DC,2015 | 13.4 | 2.8 | 3.4 | 1.6 | 6.2 | 2.9 |
| Collatuzzo G, 2023 | 21.5 | 6.2 | 1.7 | 1.85 | 0.7 | 3.75 |
| Wang JB,2012 | 22.61 | 4.40 | 0.32 | 0.27 | N/A | 29.39 |
| Teh HS, 2021 | 14.3 | 0.6 | 7.0 | 1.0 | N/A | N/A |
| Charafeddine MA, 2017 | 38.36 | 11.12 | 20 | 10.17 | N/A | 50 |
| Poirier AE, 2019 | 17.5 | 1.8 | 4.9 | 1.7 | 0.9 | 0.54 |
| Total | 23.73 | 4.87 | 7.35 | 3.73 | 5.21 | 12.27 |
Table 2 shows the PAF (%) of different variables by each study.
Discussion
Interpretation
Certain factors, such the genome or prenatal development, are regarded as "inherent" or non-modifiable risk factors for the development of cancer, meaning that people cannot control them. However, other risk variables are "modifiable," meaning that personal choices can affect things like smoking, alcohol use, physical activity, and BMI/obesity.
In this review, we concentrated on evaluating the Population Attributable Fraction (PAF) for variables that the World Cancer Research Fund (WCRF) or the International Agency for Research on Cancer (IARC) have designated as causes of cancer. Our review was further restricted to those causative factors for which exposure in the general population may be changed. Despite being somewhat arbitrary, this criterion aids in distinguishing variables like smoking, drinking, and sun exposure that may be managed by altering behavior.
Smoking
The largest population-attributable percentage (19.0% of all cases) was cigarette smoking, which was responsible for 35.0% of cancers in women and 55.5% of all possibly avoidable cancers in males6. Tobacco smoke is a known cause of cancers of the lung, bladder, renal pelvis, oral cavity, oropharynx, hypopharynx, oesophagus, larynx and pancreas, nasopharynx, nasal cavity and sinuses, stomach, kidney (body), ureter, uterine cervix, myeloid leukemia, colorectum, and ovary (mucinous), based to an IARC monograph published in 1986[12]. According to a meta-analytic research, smokers had a 2.5-fold higher chance of developing serrated polyps, and this risk rose to 3.4 times when sessile serrated adenoma/polyp risk was taken into account18. A lifetime risk of 0.2% to 1% for lung cancer may still exist for someone who has never smoked [5].
Given that males are more likely to be exposed to occupational carcinogens and have higher cumulative smoking exposure, the lack of a significant sex difference in lung cancer rates is surprising, according to a study by O'Keeffe LM et al. Along with these risky smoking habits, men also tend to smoke pipes, cigars, take longer puffs, and leave their cigarette butts shorter. Therefore, assuming their cumulative smoking exposure reaches comparable levels, it is possible that women's risk of developing lung cancer from smoking may eventually outweigh men's [19].
Alcohol
A population-attributable share of 5.6% was attributed to alcohol consumption. This suggests that alcohol use can be connected to a considerable number of health problems [6]. It has been demonstrated that excessive alcohol use, as opposed to moderate use, is responsible for a significant percentage of cancer cases [20]. Alcohol consumption has been linked to malignancies of the oral cavity, pharynx, larynx, colorectum, female breast, liver, and oesophagus (squamous cell carcinoma subtype alone), according to the IARC [68] and the WCRF [6,12]. Pooled studies for alcohol intake demonstrated a statistically significant 33% higher incidence of serrated polyp for highest versus lowest intakes [18]. An increase of 10g of ethanol per day resulted in a 5% greater chance of developing breast cancer in premenopausal women, according to a meta-analysis that established statistically significant evidence of a dose-response association between alcohol and premenopausal breast cancer risk [21].
Obesity
The IARC concluded that there was enough data to identify obesity and overweight as risk factors for malignancies of the endometrium, kidney (renal cell), colon, breast (in postmenopausal women), and oesophagus (adenocarcinoma) [6,12,22].
PAFs were higher in men than in women, and consumption of red and processed meat was linked to 5.4% and 8.2% of colorectal malignancies, respectively. Low fruit and vegetable consumption was connected with 17.6% of oral cavity/pharyngeal cancers, 17.4% of laryngeal cancers and 8.9% of lung cancers and the highest number of attributable cases was from lung cancer [6]. Meta-analyses of observational studies revealed that people who consumed the most fat and red meat had much higher risks of colorectal cancer than those who consumed the least [18].
According to a new study, having a higher BMI as a child increases the likelihood of getting cancer as an adult [22]. Being overweight or obese is one of the main factors contributing to the rising incidence and prevalence of cancer, and it may even overtake smoking as the leading avoidable cause of cancer [23].
Physical Activity
Compared to merely 1.5% of malignancies in men, 4.4% of cancers in women were caused by physical inactivity [6]. WCRF has determined that there is "convincing" or "probable" evidence linking a lack of physical exercise to endometrial, colon, and post-menopausal female breast cancers [6,12]. Breast cancer cases decreased by 23% as a result of physical activity [21]. According to one study, among people with a BMI under 25, leisure-time physical exercise was unrelated to endometrial cancer and significantly inversely correlated with lung cancer [24].
Ultraviolet Radiation
A population-attributable fraction of 4.7% was attributed to UV radiation, indicating its involvement in a number of health issues. UV radiation was the second largest contributor to all cancer cases in males and the fifth largest contributor to all cancer cases in women, despite being linked to just one type of cancer [6]. According to an IARC publication, there is enough proof that solar UV radiation causes keratinocyte malignancies (squamous cell carcinoma (SCC) and basal cell carcinoma (BCC) of the skin) and cutaneous malignant melanoma [12]. One factor influencing the induction of mutations is the pattern of UVR exposure. Despite making up only 2–3% of "UV signature mutations," BRAF mutations appear to be crucial to the genesis of cutaneous melanoma [25].
Particularly, radiation exposure has been linked to an increased risk of cancer in middle-aged individuals. Over the past 20 years, there has been a significant growth in the use of medical imaging procedures like CT and PET scans, especially among those with chronic diseases in their midlife [7]. UV light has two sides when it comes to cancer. Although UV light can produce certain beneficial compounds, such vitamin D3, and can be employed as an adjuvant therapy to treat tumors, it can also induce skin cancer [26].
Infections
We have previously demonstrated that Helicobacter pylori, high-risk human papillomavirus (HPV), hepatitis B virus (HBV), and hepatitis C virus (HCV) are the four most significant of the 11 infectious diseases that the International Agency for Research on Cancer (IARC) has designated as category 1 carcinogens [27]. Human papillomavirus (HPV), Helicobacter pylori, Epstein-Barr virus, human immunodeficiency virus, and hepatitis B and hepatitis C viruses are the primary carcinogenic pathogens. Squamous cell carcinoma of the anus, oropharyngeal cancer, and cervical cancer are all linked to HPV infections. Infections with Helicobacter pylori are closely linked to the development and spread of gastric cancer and gastric lymphoma [28].
In all, analyzed infections were responsible for 3.3% of all cancer cases. Men and women had comparable rates of gastric cancer cases linked to H. pylori infection; however, women's PAF (45.5%) was twice that of men (22.6%). HBV infection (10.5%) and HCV infection (11.6%) were similarly responsible with liver cancer in women, whereas in men, the PAF for HCV infection (28.4%) was five times higher than that for HBV (5.4%). HHV8 was identified as the cause of every Kaposi sarcoma case. The greatest number of malignancies (5440 cases) linked to HIV infection were non-Hodgkin lymphoma. HPV infection was identified as the cause of all cervical cancers (11,970 cases) and 88.2% of anal cancers (6460 cases) [6].
Conclusion and Implications for Translation
Our research concludes that the largest Population Attributable Fraction (PAF) is caused by smoking (23.73%), which is followed by infections (12.27%). Cancer development is a diverse and lengthy process that spans many years, and a life course approach becomes essential in understanding how different risk factors build over time. A vital chance to stop disease and early mortality is to concentrate on lowering modifiable risk factors. Interestingly, smoking cigarettes continues to be the leading preventable cause of cancer death. The World Cancer Research Fund (WCRF) offers important guidelines for people and populations about nutrition, physical activity, food, and alcohol use. Perhaps the easiest of these is incorporating exercise into regular activities. Additionally, changes in lifestyle, namely the move from sun avoidance to sun-seeking behaviors, have been connected to the increased prevalence of skin malignancies.
Key Message
- Our research shows that smoking causes the biggest percent of cancer cases (23.73%), underlining the importance of smoking cessation in cancer prevention.
- The World Cancer Research Fund (WCRF) guidelines suggest that nutrition, exercise, and alcohol use can lower cancer risk and early mortality.
- Skin cancers have increased as sun avoidance has given way to sun-seeking, underscoring the need for enhanced sun awareness and protection.
Declarations
Acknowledgement
We thank the researchers who posted the studies in the public domain. All authors contributed equally to this manuscript.
Ali Rohail: Conceptualization, Writing.
Javeria Tunio: Conceptualization, Methodology, Writing.
Arifa Hakro: Conceptualization, Methodology, Data Extraction.
Muhammad Ahsan: Methodology, Software, Data Extraction.
Parisa Bashir: Data Extraction, Writing.
Amina Tunio: Methodology, Data Extraction.
Funding
Nothing to declare.
Financial Disclosure
Nothing to declare.
Ethical Approval
Not applicable.
Conflicts of Interest
No conflict of interest to disclose related to this article.
Disclaimer
None.
References
- Maman S, Witz IP. (2018). A history of exploring cancer in context. Nature Reviews Cancer. 18(6):359-376.
Publisher | Google Scholor - Hassanpour SH, Dehghani M. (2017). Review of cancer from perspective of molecular. Journal of cancer research and practice. 4(4):127-129.
Publisher | Google Scholor - Badar F, Mahmood S. (2023). Cancer in Lahore, Pakistan, 2010-2019: an incidence study. BMJ Open. 11(8):e047049.
Publisher | Google Scholor - Saeed S, Khan JA, Iqbal N, Irfan S, Shafique A, et al. (2019). Cancer and how the patients see it; prevalence and perception of risk factors: a cross-sectional survey from a tertiary care centre of Karachi, Pakistan. BMC Public Health. 19:1-7.
Publisher | Google Scholor - Wu S, Zhu W, Thompson P, Hannun YA. (2018). Evaluating intrinsic and non-intrinsic cancer risk factors. Nature Communications. 9(1):3490.
Publisher | Google Scholor - Islami F, Goding Sauer A, Miller KD, Siegel RL, Fedewa SA, et al. (2018). Proportion and number of cancer cases and deaths attributable to potentially modifiable risk factors in the United States. CA: A Cancer journal for Clinicians. 68(1):31-54.
Publisher | Google Scholor - White MC, Holman DM, Boehm JE, Peipins LA, Grossman M, et al. (2014). Age and cancer risk: a potentially modifiable relationship. American Journal of Preventive Medicine. 46(3):S7-15.
Publisher | Google Scholor - Parkin DM, Boyd L, Walker LC. (2011). The fraction of cancer attributable to lifestyle and environmental factors in the UK in 2010. British Journal of Cancer. 105(2):S77-81.
Publisher | Google Scholor - Weiderpass E. (2010). Lifestyle and cancer risk. Journal of Preventive Medicine and Public Health. 43(6):459-471.
Publisher | Google Scholor - Brown KF, Rumgay H, Dunlop C, Ryan M, Quartly F, et al. (2018). The fraction of cancer attributable to modifiable risk factors in England, Wales, Scotland, Northern Ireland, and the United Kingdom in 2015. British Journal of Cancer. 118(8):1130-1141.
Publisher | Google Scholor - Grundy A, Poirier AE, Khandwala F, Grevers X, Friedenreich CM, et al. (2017). Cancer incidence attributable to lifestyle and environmental factors in Alberta in 2012: summary of results. Canadian Medical Association Open Access Journal. 5(3):E540-E545.
Publisher | Google Scholor - Whiteman DC, Webb PM, Green AC, Neale RE, Fritschi L, et al. (2015). Cancers in Australia in 2010 attributable to modifiable factors: summary and conclusions. Australian and New Zealand Journal of Public Health. 39(5):477-484.
Publisher | Google Scholor - Collatuzzo G, Boffetta P. (2023). Cancers attributable to modifiable risk factors: a road map for prevention. Annual Review of Public Health. 44(1):279-300.
Publisher | Google Scholor - Wang JB, Jiang Y, Liang H, Li P, Xiao HJ, et al. (2012). Attributable causes of cancer in China. Annals of Oncology. 23(11):2983-2989.
Publisher | Google Scholor - Teh HS, Woon YL. (2021). Burden of cancers attributable to modifiable risk factors in Malaysia. BMC Public Health. 21:1.
Publisher | Google Scholor - Charafeddine MA, Olson SH, Mukherji D, Temraz SN, Abou-Alfa GK, et al. (2017). Proportion of cancer in a Middle eastern country attributable to established risk factors. BMC Cancer. 17:1-1.
Publisher | Google Scholor - Poirier AE, Ruan Y, Volesky KD, King WD, O'Sullivan DE, et al. (2019). The current and future burden of cancer attributable to modifiable risk factors in Canada: summary of results. Preventive Medicine. 122:140-147.
Publisher | Google Scholor - Bailie L, Loughrey MB, Coleman HG. (2017). Lifestyle risk factors for serrated colorectal polyps: a systematic review and meta-analysis. Gastroenterology. 152(1):92-104.
Publisher | Google Scholor - O’Keeffe LM, Taylor G, Huxley RR, Mitchell P, Woodward M. (2018). Smoking as a risk factor for lung cancer in women and men: a systematic review and meta-analysis. BMJ Open. 8(10):e021611.
Publisher | Google Scholor - Roswall N, Weiderpass E. (2015). Alcohol as a risk factor for cancer: existing evidence in a global perspective. Journal of Preventive Medicine and Public Health. 48(1):1.
Publisher | Google Scholor - Daly AA, Rolph R, Cutress RI, Copson ER. (2021). A review of modifiable risk factors in young women for the prevention of breast cancer. Breast Cancer: Targets and Therapy. 241-257.
Publisher | Google Scholor - Tzenios N. (2023). Obesity as a risk factor for cancer. EPRA International Journal of Research and Development (IJRD). 8(2):101-104.
Publisher | Google Scholor - Avgerinos KI, Spyrou N, Mantzoros CS, Dalamaga M. (2019). Obesity and cancer risk: Emerging biological mechanisms and perspectives. Metabolism. 92:121-135.
Publisher | Google Scholor - Moore SC, Lee IM, Weiderpass E, Campbell PT, Sampson JN, et al. (2016). Association of leisure-time physical activity with risk of 26 types of cancer in 1.44 million adults. JAMA Internal Medicine. 176(6):816-825.
Publisher | Google Scholor - Greinert R, de Vries E, Erdmann F, Espina C, Auvinen A, et al. (2015). European Code against Cancer 4th Edition: Ultraviolet radiation and cancer. Cancer Epidemiology. 39:S75-S83.
Publisher | Google Scholor - Yu ZW, Zheng M, Fan HY, Liang XH, Tang YL. (2024). Ultraviolet (UV) radiation: a double-edged sword in cancer development and therapy. Molecular Biomedicine. 5(1):1-24.
Publisher | Google Scholor - de Martel C, Georges D, Bray F, Ferlay J, Clifford GM. (2020). Global burden of cancer attributable to infections in 2018: a worldwide incidence analysis. The Lancet Global Health. 8(2):e180-190.
Publisher | Google Scholor - Nagai H, Kim YH. (2017). Cancer prevention from the perspective of global cancer burden patterns. Journal of Thoracic Disease. 9(3):448.
Publisher | Google Scholor























