

Case Report
Huge Scrotum by Incarcerated Intestines with Testis Mass in A 95 Years Old Male: A Case Report
- Ahmad Reza Shahraki *
General Surgeon, Department of Surgery, Medical Faculty, Zahedan University of Medical Sciences and Health Services, Zahedan, Iran.
*Corresponding Author: Ahmad Reza Shahraki, General Surgeon, Department of Surgery, Medical Faculty, Zahedan University of Medical Sciences and Health Services, Zahedan, Iran.
Citation: Ahmad R. Shahraki. (2026). Huge Scrotum by Incarcerated Intestines with Testis Mass in A 95 Years Old Male: A Case Report, Clinical Case Reports and Studies, BioRes Scientia Publishers. 12(3):1-6. DOI: 10.59657/2837-2565.brs.26.303
Copyright: © 2026 Ahmad Reza Shahraki, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: January 26, 2026 | Accepted: February 12, 2026 | Published: March 16, 2026
Abstract
This case report has reported in line with the SCARE Criteria. Large testicular tumor is not a commonly seen entity in the modern era. While treatment of large testicular tumors is via inguinal radical orchiectomy, large testicular tumors carry the dilemma of delivering these large masses via the inguinal or scrotal approach.
Our case was a 95 years old man with obstruction signs and huge scrotum that shows incarcerated large bowel with huge testicular mass, that in his surgery, we did Radical Orchiectomy and we replace incarcerated Large Bowel in scrotum and discharge him successfully. Giant testicular cancer is considered one of the largest testicular masses in the world. Delayed seeking medical advice and appropriate management is the major cause behind this rare presentation. Increasing the awareness regarding self-examination and eliminating the stigma is the cornerstone to markedly reduce this type of unusual presentation since any testicular size change and mass can be easily noted by the patient.
Surgical exploration and adjuvant chemotherapy seems as a reasonable treatment option in the setting of bilateral intra-abdominal testis tumor in an adult patient. The study underscores the effectiveness of the intervention in promoting preventive behaviors against testicular cancer among university students, laying the groundwork for future educational initiatives. Although testicular cancer (TC) is the most common malignancy in males between the ages of 18 and 50 years, little effort has been made to increase public awareness about TC and testicular self-examinations (TSEs). Intestinal obstruction without a past surgical history of abdominal surgeries or trauma is a rare and challenging clinical situation. This case report describes the presentation, diagnosis, and management of intestinal obstruction in a patient with an uncommon etiology of small bowel obstruction. Chronic hernia incarceration can lead to weakening and ischemia of the bowel, and minimal trauma can lead to perforation of the weakened segment. In such presentations, bowel resection and repair of the defect with a biological material is safe and feasible. Surgery remains the mainstay of treatment and early intervention improves the chances of a favorable outcome. In old person, we can find appendix and diseases related to it.
Keywords: sarcoma; large bowel; mass; testis; tumor; testicular cancer; incarcerated bowel; intestinal obstruction; case report
Introduction
Large testicular tumor is not a commonly seen entity in the modern era. While treatment of large testicular tumors is via inguinal radical orchiectomy, large testicular tumors carry the dilemma of delivering these large masses via the inguinal or scrotal approach [1]. Testicular cancer is considered a rare malignancy globally; in this regard, testicular cancer is appraised as a disease of young and adult men. Although it can manifest in childhood with a reported percentage of 7%, the mean age of incidence in general population is between the ages of 20 and 34 years [2]. Considerable risk factors such as age, ethnicity, family history of testicular cancer, and cryptorchidism are acknowledged as well [3]. Testicular germ cell tumors (TGCTs) are the most frequently encountered type of testicular cancer. Histologically, TGCTs are categorized into three categories: seminomas, nonseminomas, and spermatocytic seminomas with the seminomas and
nonseminomas count as the majority of TGCT as much as 98%–99% [4]. Testicular cancer may present in different ways such as painless scrotal swelling, incidental finding in radiological imaging, and posttraumatic or metastatic symptoms. As that as it may be, the U.S. Preventive Task Force opposes screening for testicular cancer in asymptomatic young and adult patients with no testicular cancer risk. However, the American Cancer Society does recommend testicular examination as part of the routine cancer-related checkup (4). Presence of any kind of solid mass in the testis should it be identified by physical examination, or imaging is ought to be managed as a malignancy until proven otherwise [5]. The AUA guideline promotes the investigation of any suspicious solid mass in the testis with initial imaging by Doppler ultrasound and serum tumor markers, which consist of alpha-fetoprotein (AFP), human chorionic gonadotropin (hCG), and lactate dehydrogenase (LDH). Findings of hypoechoic mass with vascular flow on the US investigation is highly skeptical of testicular conserve [5]. The standardized initial management of unilateral testicular cancer at the existence of normal contralateral testis is radical inguinal orchiectomy (4). An attempt of taking trans-scrotal testicular biopsy should not be carried out as it may disturb the lymphatic drainage of the tumor and spoil the scrotum. The sample of the radical inguinal orchiectomy must be sent for histopathological interpretation [6]. Testicular cancer treatment and prognosis plan is made in multi-multidisciplinary structure formula that involves histopathology, clinical staging, prognosis of the disease, and specialist–patient debate on positive and negative outcomes of the treatment. However, adjusted modified treatment plans based on risk-adapted therapy in nonseminoma patients are yet to prove its worth seminoma patients [3]. Intestinal obstruction without a past surgical history of abdominal surgeries or trauma is a rare and challenging clinical situation. This case report describes the presentation, diagnosis, and management of intestinal obstruction in a patient with an uncommon etiology of small bowel obstruction [17]. Some cases can be successfully treated with emergent laparoscopic surgery [18].
Case Presentation
Our case was a 93 years old man that referred to surgery part with abdominal pain, we admit him and start examination, we find huge scrotum that was carried for 2 days (figure1).

Figure 1: Huge scrotum
We continue our assessment and we find sign and symptoms of intestinal obstruction and did Ultrasonography that shows bowel in scrotum and we prepare him for surgery with incarcerated intestine with inguinal approach (figure2).

Figure 2: Incarcerated intestine
With continuous surgery to check testis we find a testicular mass that puled intestine into the scrotum (figure3).
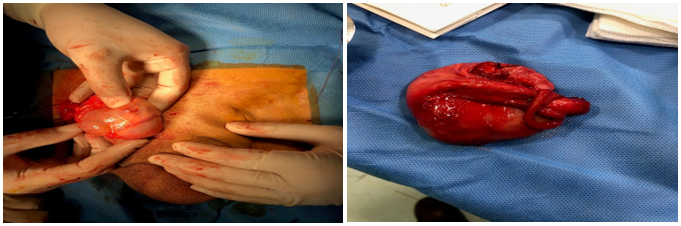
Figure 3: Testicular Mass
We did Radical orchiectomy by inguinal approach and replace intestine in abdomen and repair inguinal hole by tissue flap. After 2 days patient has defecation and we discharge him healthy and successfully.
Discussion
The advances seen in the treatment of testicular cancer are among the great achievements in modern medicine. These advances were made possible by the collaborative efforts of cancer researchers around the world. Investigators have been able to address many questions regarding the treatment of patients with disease limited to the testis, those with metastasis to the retro peritoneum only, and those with advanced metastatic disease. Questions answered include the chemotherapeutic agents to be used and in what combinations, the proper intensity of treatment and appropriate dosing, the optimal number of cycles of chemotherapy according to validated risk stratification, appropriate surgical approaches that preserve sexual function, the treatment of relapsed disease, what supportive care measures to take, and survivorship issues following treatment of testicular cancer. Today, cure is achievable in 95% of all patients with testicular cancer and 80% of those who have metastatic disease. Despite remarkable results with frontline and salvage combination chemotherapy, metastatic testicular cancer remains incurable in approximately 10% of patients, and novel treatment approaches are warranted. This review highlights past and recent discoveries in the treatment of patients with testicular cancer [6]. Testicular cancer is the most common type of malignancy in young adult males, accounting for 1 % of all cancer diagnosis in men and 5 % of all urologic tumors. It is one of the malignancies with the highest cure rate. Bilateral germ cell tumor of the testicles is rare, representing only 1 % of all new cases of testicular cancer, around 30 % of which occur synchronously. Interestingly, there is not yet an occurrence where the bilateral synchronous testicular cancer has different histopathological type [7]. Known risk factors for testicular cancers include cryptorchidism, prior testicular germ cell tumor (TGCT), having a father with TGCT, having a brother with TGCT, and higher body height. Prior testicular germ cell tumor (TGCT) and higher body height are the risk factors that are found in this patient's case. Among these factors, the greatest relative risk is having a brother with testicular TGCT, increasing the individual's risk by approximately 10 times (RR 7.55–12.74, 95 % CI), followed by history of cryptorchidism (RR 4.3, 95 % CI) [8]. A review of the related literature in recent years reveals several reports of TMGCTs manifesting with fever and lymph node enlargement, which may be explained by the undetectable onset of the disease as well as limited knowledge of the disease to date. The diagnostic process and treatment plan for this patient may serve as a reference in clinical practice [10]. Giant testicular cancer is considered one of the largest testicular masses in the world. Delayed seeking medical advice and appropriate management is the major cause behind this rare presentation. Increasing the awareness regarding self-examination and eliminating the stigma is the cornerstone to markedly reduce this type of unusual presentation since any testicular size change and mass can be easily noted by the patient [11]. This case report has been reported in line with the SCARE Criteria [26]. Increasing the awareness regarding self-examination and eliminating the stigma is the cornerstone markedly reduce this type of unusual presentation since any testicular size change and mass can be easily note by the patient [27].
Conclusion
Giant testicular cancer is considered one of the largest testicular masses in the world. Delayed seeking medical advice and appropriate management is the major cause behind this rare presentation. Increasing the awareness regarding self-examination and eliminating the stigma is the cornerstone to markedly reduce this type of unusual presentation since any testicular size change and mass can be easily noted by the patient. Treatment with surgery and chemotherapy is well tolerated and received. A further specific clinical study needs to be performed to investigate this finding in the future [7]. Surgical exploration and adjuvant chemotherapy seems as a reasonable treatment option in the setting of bilateral intra-abdominal testis tumor in an adult patient [9]. Giant testicular cancer is considered one of the largest testicular masses in the world. Delayed seeking medical advice and appropriate management is the major cause behind this rare presentation. Increasing the awareness regarding self-examination and eliminating the stigma is the cornerstone to markedly reduce this type of unusual presentation since any testicular size change and mass can be easily noted by the patient [11]. In conclusion, the present case report underscores the rarity and slow-growing nature of testicular ScTs, emphasizing the significance of prompt identification and treatment. Clinical examination, tumor markers, and imaging techniques are vital for accurate diagnosis. Radical orchiectomy is crucial for ensuring favorable outcomes, and long-term monitoring is necessary to detect any potential recurrence or spread [12]. The study underscores the effectiveness of the intervention in promoting preventive behaviors against testicular cancer among university students, laying the groundwork for future educational initiatives [13]. Our data on testicular GCT including demographic, histological, and treatment outcomes were comparable to that of developed countries. In light of the pathology discrepancy rate revealed in our study, authors recommend a second review by expert genitourinary pathologists to ensure proper classification and management of GCT (14). Mixed germ cell tumors with choriocarcinoma components are rare and tend to affect younger populations. These tumors demonstrate aggressive clinical behavior, with a significant proportion presenting with high-grade lesions and metastasis at diagnosis. The observed mortality rate underscores the poor prognosis associated with this malignancy [15]. Although testicular cancer (TC) is the most common malignancy in males between the ages of 18 and 50 years, little effort has been made to increase public awareness about TC and testicular self-examinations (TSEs) [16]. The importance of considering rare etiologies in patients with abdominal pain, especially those lacking a typical history, is emphasized. The effective use of imaging and tailored surgical approach was key to the successful outcome. This report adds to the limited literature on omental breaches causing intestinal obstruction and underlines the necessity of a multidisciplinary approach in such cases [17]. Some cases can be successfully treated with emergent laparoscopic surgery [18]. Chronic hernia incarceration can lead to weakening and ischemia of the bowel, and minimal trauma can lead to perforation of the weakened segment. In such presentations, bowel resection and repair of the defect with a biological material is safe and feasible [19]. Generally, some problem can affect on this situation: The discussed case is extremely rare. The case’s novelty is that it is a true hernia in an orthopedic surgery wound of the iliac wing ORIF, the clinical presentation and the surgical treatment used. There are not enough data about the epidemiology, prognosis or treatment guidelines. Reviewing the previous literature, we did not find any article describing a similar condition [20]. In herniorrhaphy with mesh, minimization of bowel resection is important for preventing postoperative infection of the mesh. In this case, ICG fluorescence with a near-infrared fluorescence camera was central to reducing bowel resection [21]. Giant testicular cancer is considered one of the largest testicular masses in the world. Delayed seeking medical advice and appropriate management is the major cause behind this rare presentation. Increasing the awareness regarding self-examination and eliminating the stigma is the cornerstone to markedly reduce this type of unusual presentation since any testicular size change and mass can be easily noted by the patient [22]. A follow-up CT showed reduction in the metastasis size and numbers despite this; the hCG and LDH levels have risen from the initial numbers which probably indicate a partial response [23]. Surgery still remains the mainstay of treatment and early intervention improves the chances of a favorable outcome [24].
In old person, we can find appendix and diseases related to it [25].
Declarations
Ethical Approval and Consent to participate
The content of this manuscript is in accordance with the declaration of Helsinki for Ethics. No committee approval was required. Oral and written consent to participate was granted by the parents.
Consent for publication
“Written informed consent was obtained from the patient's legal guardian for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.”
Availability of supporting data
It is available.
Competing interests
The author declares that they have no competing financial interests and nothing to disclose.
Funding
There is no funding.
Authors' contributions
Ahmad Reza Shahraki was the surgeon of patient and writes this paper.
The author declares that they have no competing financial interests and nothing to disclose.
Acknowledgements
In abdomen, you can face with verified problem and should notice to scrotum in examination of patient with abdominal pain. In old person, we can find appendix and diseases related to it.
Authors' information
Ahmad Reza Shahraki
1-Assistant professor, Department of surgery, Zahedan medical faculty, Zahedan University of medical Sciences, Zahedan, Iran.
References
- Alaskari, M. M., Hassan, I. A. B., Aldakhil, T. A., & Al Khatem, R. S. (2023). A case report of large testicular mass: An Eastern Province report from KSA. Urology Annals, 15(1):101–103.
Publisher | Google Scholor - Abomelha, M. (2017). Adult testicular cancer: Two decades of Saudi national data. Urology Annals, 9(4):305–309.
Publisher | Google Scholor - Baird, D. C., Meyers, G. J., & Hu, J. S. (2018). Testicular cancer: Diagnosis and treatment. American Family Physician, 97(4):261–268.
Publisher | Google Scholor - Ghazarian, A. A., Trabert, B., Devesa, S. S., & McGlynn, K. A. (2015). Recent trends in the incidence of testicular germ cell tumors in the United States. Andrology, 3(1):13–18.
Publisher | Google Scholor - Stephenson, A., Eggener, S. E., Bass, E. B., Chelnick, D. M., Daneshmand, S., Feldman, D., Gilligan, T., Karam, J. A., Leibovich, B., Liauw, S. L., Masterson, T. A., Meeks, J. J., Pierorazio, P. M., Sharma, R., & Sheinfeld, J. (2019). Diagnosis and treatment of early stage testicular cancer: AUA guideline. Journal of Urology, 202(2):272–281.
Publisher | Google Scholor - Adra, N., & Einhorn, L. H. (2017). Testicular cancer update. Clinical Advances in Hematology & Oncology, 15(5):386–396.
Publisher | Google Scholor - Ginting, J. T., Sihombing, B., Warli, S. M., Siregar, G. P., & Prapiska, F. F. (2023). Bilateral synchronous testicular cancer: A case report. International Journal of Surgery Case Reports, 103:107870.
Publisher | Google Scholor - Campobasso, D., Ferretti, S., & Frattini, A. (2017). Synchronous bilateral testis cancer: Clinical and oncological management. Contemporary Oncology (Poznan), 21(1):70–76.
Publisher | Google Scholor - Sandikci, F., Cimen, S., Cimen, S. G., Imamoglu, G. I., Han, U., Kokurcan, A., Baylan, B., Goktug, G., & Imamoglu, A. (2018). Bilateral intra-abdominal testicular tumor: Case report. International Journal of Surgery Case Reports, 49:102–105.
Publisher | Google Scholor - Xiao, Q. F., Li, J., Tang, B., & Zhu, Y. Q. (2023). Testicular mixed germ cell tumor: A case report. World Journal of Clinical Cases, 11(28):6902–6907.
Publisher | Google Scholor - Bapir, R., Aghaways, I., Ali, R. M., Fakhralddin, S. S., Rashid, R. J., Abdullah, A. M., Ali, M. A., Mohammed, K. K., & Abdullah, H. O. (2023). Spermatocytic tumor of the testis: A case report and mini review of the literature. Medical International, 3:51.
Publisher | Google Scholor - Ibrahim, A. M., & Fathi Zaghamir, D. E. (2024). Enhancing testicular cancer prevention among university students: A health belief model and social support intervention. Asian Pacific Journal of Cancer Prevention, 25(2):609–616.
Publisher | Google Scholor - El-Achkar, A., Alasadi, H., El-Asmar, J., Armache, A., Abu-Hijlih, R., Abu-Hijle, F., Al-Ibraheem, A., Khzouz, J., Salah, S., & Shahait, M. (2023). Clinical characteristics and treatment outcomes of germ cell tumor in Jordan: A tertiary center experience. Arab Journal of Urology, 21(4):233–239.
Publisher | Google Scholor - Al-Khayal, A., Noureldin, Y., Alghafees, M., Shafqat, A., Sabbah, B. N., Elhossiny, A. H., Bakir, M., Omar, M. A., Arabi, T. Z., Abdul Rab, S., Alsaikhan, B., Aldhalaan, R., Alquirnas, M., & Alrabeeah, K. (2023). A decade in focus: Mixed germ cell tumors with choriocarcinoma components. Annals of Medicine and Surgery, 85(11):5355–5358.
Publisher | Google Scholor - Alkhayal, A., Alsaikhan, B. H., Alhajress, G., Alsaghyir, A., Noureldin, Y. A., Aldraihem, K., & Alrabeeah, K. (2023). Perceptions of testicular cancer and self-examination in the general population of Saudi Arabia. Urology Annals, 15(3):266–270.
Publisher | Google Scholor - Chaouch, M. A., Taieb, A. H., Jallali, M., Chedly, E., Gafsi, B., & Noomen, F. (2024). Rare case report of intestinal obstruction due to incarcerated small bowel in omental breach. International Journal of Surgery Case Reports, 115:109245.
Publisher | Google Scholor - Hakiman, H., DeLibero, J., & Pham, T. (2013). Coughing-induced bowel transection in a patient with an incarcerated inguinal hernia: A case report. Journal of Medical Case Reports, 7:47.
Publisher | Google Scholor - Abu-Jeyyab, M., Al-Jafari, M., AlKhawaldeh, I. M., Zein Eddin, S., Abu Tapanjeh, S., Ja’Awin, M., Aborajooh, E., & Nashwan, A. J. (2024). Incarcerated incisional hernia on an old orthopedics incision: A rare case report and a review of the literature. Journal of Surgical Case Reports, 2024(5):rjae369.
Publisher | Google Scholor - Ryu, S., Yoshida, M., Ohdaira, H., Tsutsui, N., Suzuki, N., Ito, E., Nakajima, K., Yanagisawa, S., Kitajima, M., & Suzuki, Y. (2016). A case of incarcerated femoral hernia with intestinal blood flow assessment by brightfield full-color near-infrared fluorescence camera: Report of a case. International Journal of Surgery Case Reports, 29:234–236.
Publisher | Google Scholor - Jackson, S. R., Koestenbauer, J., Samra, S., & Indrajit, B. (2020). Giant testicular tumour with major choriocarcinoma component. Urology Case Reports, 32:101234.
Publisher | Google Scholor - Igbokwe, M. C., Badmus, T. A., Salako, A. A., David, R. A., Aigbe, E., Laoye, A., & Akinbola, I. A. (2018). Scrotal squamous cell carcinoma and associated blindness: A case report and literature review. Journal of the West African College of Surgeons, 8(3):106–113.
Publisher | Google Scholor - Shahraki, A. R. (2024). Acute appendicitis in a 95 years old male patient: uncommon age for a common disease, a case report and review of literature. Chronicles of Clinical Reviews and Case Reports, 1:1–8.
Publisher | Google Scholor - Agha, R. A., Franchi, T., Sohrabi, C., & Mathew, G. (2020). The SCARE 2020 guideline: Updating consensus surgical CAse REport (SCARE) guidelines. International Journal of Surgery, 84:226–230
Publisher | Google Scholor























