

Research Article
Effectiveness of Aligner Technique in Space Closure Compared to The Edgewise Technique: Systematic Literature Review
1Dentist, Postgraduate Resident of Orthodontics, Pontificia Universidad Javeriana, Bogotá, Colombia.
2Dentist, Specialist in Orthodontics, Postgraduate Director of Orthodontics, Pontificia Universidad Javeriana, Bogotá, Colombia.
3Dentist, Specialist in Epidemiology, Mg. In Public Health, Undergraduate-Postgraduate Professor, Pontificia Universidad Javeriana, Bogotá, Colombia.
*Corresponding Author: María Fernanda García, Dentist, Postgraduate Resident of Orthodontics, Pontificia Universidad Javeriana, Bogotá, Colombia.
Citation: García MF, Guisande MV, Valenzuela P, Suárez A. (2026). Effectiveness of Aligner Technique in Space Closure Compared to The Edgewise Technique: Systematic Literature Review, International Journal of Biomedical and Clinical Research, BioRes Scientia Publishers. 6(2):1-15. DOI: 10.59657/2997-6103.brs.26.114
Copyright: © 2026 María Fernanda García, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: December 29, 2025 | Accepted: January 20, 2026 | Published: January 30, 2026
Abstract
Background: Clear aligners are a highly aesthetic alternative for orthodontic correction of malocclusions. However, when it comes to their effectiveness in space closure compared to the edgewise technique, the results reported in the literature are controversial.
Objective: Determine the effectiveness of the aligner technique in space closure compared to the edgewise technique through a systematic literature review.
Materials and Methods: Electronic and manual search in databases using controlled and uncontrolled language. Publications between January 1999 and August 2022, corresponding to intervention studies and analytical observational studies (cohort and case-control), with no language restrictions. The methodological quality, level of evidence, and degree of recommendation of the included studies were evaluated, and the results were synthesized in an analysis matrix.
Results: Both techniques were effective in reducing space in millimeters (residual space of 1 mm up to complete closure). The total treatment time was shorter in patients with Invisalign® compared to the edgewise technique. However, in extraction cases, it was reported that treatment time is 44% longer with Invisalign®. Regarding the predominant type of movement in space closure, a coronal tipping into the space with the edgewise technique, while there is a progressively tipping of teeth into spaces in small increments with aligners. The success rate in relation to the overall effectiveness of dental movement was 59%. There is no difference between both groups in terms of gingival effects during space closure. Regarding secondary effects, lingual/palatal crown torque of the anterior segment was highlighted during closure in both techniques. Pain perception was lower with aligners. According to the VAS, during the first month, there was a lower pain perception with aligners, and from months 2 to 12, the pain was higher.
Conclusion: The publications analyzed in this review demonstrated that space closure in millimeters with aligners is equally effective as that achieved with edgewise technique.
Keywords: effectiveness; conventional orthodontics; aligners; invisible aligners; invisalign®, space closure; orthodontic space closure; permanent dentition; pain; gingival effects
Introduction
Aligners are transparent devices that fit the contour of the patient's teeth, composed of a thermoplastic material such as the glycol-modified polyethylene terephthalate (PET-G), polypropylene, polycarbonate (PC), thermoplastic polyurethanes (TPU), ethylenvinylacetate, methylene diphenyl disyncyanate and 1,6-hexanediol, among others. These must be transparent, with low hardness, good elasticity, high resistance, biocompatible, comfortable, aesthetic, and effective in the correction of malocclusions; allowing progressive movements without the need for brackets [1,2]. Originally, they were only considered for mild or moderate malocclusions, being limited to the correction of crowdings [3]; however, they have become a more versatile option due to the high aesthetics, comfort and ease of hygiene they offer, which represents the main demand of those who seek this treatment [2,4].
Orthodontic treatment with aligners has demonstrated an effectiveness (difference between initial and final Clincheck) average of 50% for all dental movements, and it has been determined that the oro-lingual inclination of the crown is the most effective movement, reaching 56%. In relation to PAR index scores, post-treatment, Gu et al. (2017) [5] have shown that aligners are highly successful in improving anterior tooth alignment, transverse relationships, and vertical overbite; moderately successful in improving midline and horizontal overbite, and less successful in improving posterior occlusion.
Authors such as Lanteri et al. (2018) [6] and Gaffuri et al. (2020) [7], argue that, despite the boom in its use, the evidence on the effectiveness of the technique is not representative with respect to alignment and leveling, and the closure of spaces, which raises the debate about whether it is capable of achieving necessary movements in some clinical situations. For their part, Dai et al. (2021) [8] The limitations in the use of aligners to close the extraction space in cases with extractions stand out, due to the difficulty in maintaining their original shape during the distalization of the teeth involved. In their review, Simon et al. (2014) [9] and Ravera et al. (2016) [10] they mention that the precision of body movement with aligners is limited; especially in patients who require the closure of spaces or extractions. Similarly, Dai et al. (2019) [11], Gaffuri et al. (2020) [7], and Dai et al. (2021) [8] have reported a limitation of studies that delve into the biomechanics involved, the functioning of the attachments and the movements that occur during the closure of spaces, both in individuals who require extractions and in those who do not [7-11].
The growing development of the aligner technique and its attachments has allowed a higher overall success rate, of up to 74%, in the management of patients who require various dental movements; however, there is no clarity about the ability of the technique to achieve the closure of spaces [12]. Dai et al. (2021) [8] reported better control of crown movement in patients requiring space closure, presenting only mild Tip mesial, in the teeth adjacent to space; however, anteroposterior displacement of the teeth involved was not achieved as predicted.
On the other hand, aligner treatment differs from the arch technique because of the large contact surface between the teeth and the device. In the arch ridge technique, the single point of contact is at the base of the bracket, while the aligners cover the entire clinical crown and part of the gingival edge [13]. This difference raises questions about its effects on periodontal tissue, the pain it can cause to the patient, and the consequences on occlusion. Miethke et al. [13] they showed that those treated with aligners do not present a greater periodontal risk, despite the fact that the teeth and part of the gingival tissue are covered most of the day by the aligners; Lanteri et al. (2018) [6]. They delve into the incidence of gingival recessions during treatment with both techniques. For their part, Antonio, et al. (2019) [14], mention that pain with Invisalign® is less than with the arch technique during the first month of treatment. With this, the need to investigate the biomechanics required to achieve effective space closure using aligners has been determined, to ensure that the desired movements conform to the established treatment plan [8].
The objective of the present study was to determine the effectiveness of aligner treatment in patients with permanent dentition during space closure, compared to the orthodontic arch technique, based on evidence-based medicine. It should be considered that, for the purposes of this systematic review of the literature, the term effectiveness will be measured as the reduction in space in millimeters (mm) achieved in each of the groups (aligners and orthodontics with the arch technique of edge).
Materials and Methods
The present research was developed from an integrative study, whose design was related to a systematic review of the literature, which sought to answer the following research question, using the "PICO" structure: In individuals with permanent dentition, in orthodontic treatment, who require the closure of spaces, is the technique with aligners as effective as the orthodontic technique with an arch of edge?
The object of study was related to the effectiveness of the aligner technique in closing spaces. The observation unit was linked to primary sources published in the period between January 1, 1999 and August 31, 2022, whose study population was related to individuals who had permanent dentition, with the need to close spaces, using the aligner technique or the arch technique [where the two techniques were compared, regardless of the stage of treatment]. Publications without language discrimination were included. The search included intervention study designs: (controlled clinical trials, non-controlled trials), intervened case series; analytical observational studies: case-controls (whose exposure was related to treatment), prospective and retrospective cohort studies. Scientific publications were excluded where patients with active periodontal disease, systemically compromised patients, and syndromic patients were reported.
Procedure
An electronic search was carried out in the databases: PubMed, Scopus, Web of Science, Embase, Cochrane and Dentistry and Oral Sciences Source, Scielo, and through Google Scholar using search descriptors in controlled and uncontrolled language; additionally, a manual search was performed. Bolean operators AND, OR and NOT were used, characterizing the search formulas according to the particularities of each database (Table 1). The complete formulas are included as an annex at the end of the text (Annex 1).
Table 1: Main database search strategy.
| Databases | Selected Search Strategies |
| Embase | ('human'/exp OR human) AND ('secondary dentition'/exp OR "secondary dentition') AND ('orthodontic aligner'/exp OR 'orthodontic aligner') AND ('orthodontic bracket/exp OR 'orthodontic bracket') AND ('clinical effectiveness/exp OR 'clinical effectiveness') OR 'orthodontic space closure'/exp OR 'orthodontic space closure' |
| PubMed | ((((((((PEOPLE) OR (PERSONS)) OR (ADULTS)) OR (HUMANS) ) OR (ORTHODONTIC PATIENTS) AND (adolescent(Filter) OR alladult[Filter] OR youngadult(Filter) OR adult(Filter) OR middleagedaged[Filter] OR middleaged[Filter] OR aged[Filter] OR 80andover[Filter])) AND (((PERMANENT DENTITION) OR (SECONDARY DENTITION)) OR (ADULT DENTITION) AND (adolescent[Filter] OR alladult(Filter] OR youngadult[Filter] OR adult[Filter] OR middleagedaged[Filter] OR middleaged[Filter] OR aged[Filter] OR 80andover[Filter]))) AND ((((((((((((((CLEAR ALIGNER APPLIANCES) OR (ALIGNER APPLIANCE)) ) OR (ALIGNER APPLIANCES)) OR (CLEAR ALIGNER)) OR (CLAR ALIGNER APPLIANCE)) ) OR (ORTHODONTIC REMOVABLE APPLIANCES)) OR (DENTAL ALIGNERS)) OR (INVISALIGN)) OR (INVISALIGN ORTHODONTICS)) OR (INVISALIGN TREATMENT)) OR (INVISALIGN APPLIANCE) AND (adolescent[Filter] OR alladult(Filter) OR youngadult(Filter) OR adult[Filter] OR middleagedaged[Filter] OR middleaged[Filter] OR aged[Filter] OR 80andover[Filter]))) AND (((((((ORTHODONTIC BRACKETS) OR (BRACKETS)) OR (BRACES)) OR (DENTAL BRACES)) OR (EDGEWISE TECHNIQUE)) OR (CONVENTIONAL ORTHODONTIC TREATMENT)) OR (BRACES TREATMENT) AND (adolescent[Filter] OR alladult[Filter] OR youngadult[Filter] OR adult[Filter] OR middleagedaged[Filter] OR middleaged[Filter] OR aged[Filter] OR 80andover[Filter]))) AND ((EFFECTIVENESS)) OR (COMPARATIVE EFFECTIVENESS RESEARCH)) OR (SPACE CLOSURE EFFECTIVENESS)) OR (ORTHODONTIC SPACE CLOSURE) AND (adolescent(Filter) OR alladult(Filter) OR youngadult[Filter] OR adult[Filter] OR middleagedaged[Filter] OR middleaged[Filter] OR aged[Filter] OR 80andover[Filter])) |
| Ebsco | people OR adults AND permanent dentition OR adult dentition AND aligners OR clear aligners OR clear aligner therapy OR [clear aligner appliances]] AND orthodontic braces AND effectiveness AND orthodontic space closure |
| Scopus | person OR human AND secondary AND dentition OR permanent AND dentition AND clear AND aligner OR orthodontic AND aligner AND effectiveness OR orthodontic AND space AND closure |
| Web of Science | ((((ALL=(people)) OR ALL=(persons)) OR ALL=(adults)) OR ALL=(humans)) OR ALL=(orthodontic patients) AND (ALL=(permanent dentition)) OR ALL=(secondary dentition) AND (((((ALL=(aligners)) OR ALL=(clear aligners)) OR ALL=(clear aligner appliance )) OR ALL=(orthodontic removable appliance)) OR ALL=(aligner appliances)) OR ALL=(5linico5gn) AND ((ALL=(orthodontic brackets)) OR ALL=(orthodontic braces)) OR ALL=(fixed orthodontic appliances)) OR ALL=(brackets)) OR ALL=(braces)) OR ALL=(corrective orthodontics)) OR ALL=(dental brace)) OR ALL=(conventional orthodontic treatment) AND (((ALL=(comparative effectiveness research)) OR ALL=(orthodontic space closure)) OR ALL=(space closure)) OR ALL=(space closure effectiveness) |
| Scielo | (*Humans) OR (people) OR (persons) OR (adults) OR (orthodontic patients) AND (permanent dentition) OR (secondary dentition) AND (aligners) OR (clear aligners) AND (orthodontic brackets) OR (brackets) OR (braces) OR (fixed orthodontic appliances) AND (comparative effectiveness research) OR (space closure) OR (orthodontic space closure) OR (space closure effectiveness) |
| Cochrane | people OR persons OR humans OR orthodontic patients OR adults AND permanent dentition OR secondary dentition AND comparative effectiveness research OR space closure OR orthodontic space closure OR space closure effectiveness |
From the initial search, duplicate publications were excluded, through the Rayyan QCRI platform. Subsequently, the titles and abstracts were reviewed, continuing with the verification of the eligibility criteria and the subsequent reading of the full texts. The determination of methodological quality was carried out through the checklists: Consort (randomized controlled clinical trials), Trend (non-controlled clinical trials), Care (intervened case series), Strobe (retrospective observational analytical, cohort and case-control designs) and generic Strobe (observational analytical prospective cohort and observational analytical, ambispect observational designs). Subsequently, the level of evidence and the degree of recommendation of the publications were identified based on the Oxford guide.
The systematization process was reported in a flowchart (Figure 1). The publications included in the final filter were analyzed, based on a bibliographic matrix, including aspects related to: title of the article, author, date of publication, general objective, study design, population, variables analyzed, results, conclusions, level of evidence and degree of recommendation. Based on these results, we sought to answer the following units of analysis: effectiveness of aligners in closing spaces; success rate expressed as a percentage (based on the intervals identified by the authors of the publications); reduction of space closure (expressed in millimeters); time of closure of spaces (expressed in months); pain perception, gingival architecture and side effects of closure. Independent variables were related to the type of technique (ridge arch aligners); age behavior and time since extraction were identified as possible confounding variables. The protocol record in PROSPERO is identified with the number CRD42023352563.
Results
Once the systematization process was carried out, the final filter included 12 publications. (Figure 1) The selected articles corresponded to: 4 randomized controlled clinical trials, 2 non-randomized clinical trials, 1 intervened case series, 1 retrospective cohort analytical observational study, 1 prospective cohort analytical observational study, 2 case-control analytical observational studies, 1 ambispective analytical observational study.
The synthesis of the characteristics of the publications included in the final filter is presented in Table 2.
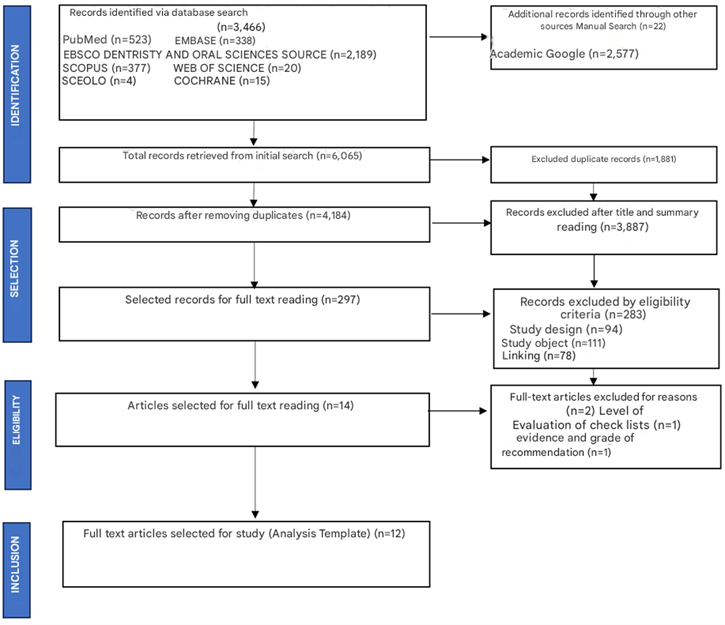
Figure 1: Systematization flowchart.
Table 2: Final filter publication results synthesis matrix: (n=12).
Units of Analysis
The results were summarized in Table 2; however, they are developed in greater detail below according to the units of analysis that were taken into account for the development of the review, highlighting the main findings, in order to respond to each of the objectives initially proposed.
Reduction of Space in Millimeters
Of the 12 articles, 33.3% (n=4) refer to the reduction of space in millimeters, comparing the two techniques. Three publications reported that this the reduction was similar in both groups [5,17,23] Lin et al. (2021) [17] mentioned that the two techniques obtained similar results at the close of spaces for T1 (post-treatment) and T2 (after 6 months of retention) according to the OGS score, for interproximal contacts; this being 0 points, which indicates that they managed to make the interproximal space ≤0.5 mm. For its part, Koumpia et al. (2008) [23] They reported that the lowest average score (fewer points lost) was that of interproximal contacts for both groups, indicating that there was no statistically significant difference between them. On the other hand, Gu, et al. (2017) [5] mentioned that, regarding the post-treatment PAR Index scores for the alignment variables of the previous segment, there were no statistically significant differences between both groups. In both components and in both groups, the displacement of the point of contact in most cases obtained a score of 0 (0-1 mm), being the best score according to the PAR Index. These scores range from 0 to 5, with 0 having the least displacement from the point of contact and 5 having the highest displacement [5]. Djeu et al. (2005) [19], identified that the Invisalign® group had a greater loss of points for interproximal contacts compared to the ideal standard set by the ABO; although this difference was not statistically significant with the orthodontic technique of arching edge. The authors mentioned that aligners can produce adequate gap closure of up to 6 mm in total [19].
Time Behavior, In Months, For the Closure of Spaces
Of the total number of articles selected, 58.3% (n=7) refer to the time in months of treatment, comparing the two techniques. Five publications mentioned that the total treatment time was shorter in patients with Invisalign® (approximate lapse of 11.5-19.52 months) compared to the arching technique (approximate lapse of 17-23.62 months) [5,16,19,21,22]. However, Lin. et al. (2021) [17] refer to the fact that the total duration of treatment was longer in patients with Invisalign® (19 months) compared to the orthodontic arching technique (15 months). In addition, Koumpia et al. (2008) report that no statistically significant differences were found in the duration of treatment between the two groups. Additionally, Christou et al. (2020) [21] They highlight that in those patients who need extractions, it has been reported that treatment with Invisalign® is 44% longer than treatment with an arch of edge.
Type of Movement Predominant in The Closing of Spaces
Three articles (n=3) evaluated the type of movement predominant in the closing of spaces. Djeu et al. (2005) [19] They mentioned that those patients treated with aligners consistently presented adequate space closure, with the progressive inclination of the teeth adjacent to the edentulous space being observed in small increments. This study highlighted the difference in orolingual tilt, as the Invisalign® group lost more points on the OGS than the arch-edge orthodontic group on average; and reiterates that the highlights of Invisalign® were its ability to close gaps, and correct for previous rotations and marginal ridge heights [19].
On the other hand, Lin. Et al. (2021) [17] reported that after treatment, Invisalign® had better scores of Root alignment and angulation than the singing bow. In this regard, Antonio, et al. (2019) [14] mentioned that to improve tooth movement during the closure of spaces with Invisalign®, it is necessary to use other devices such as microscrews or power arms due to the complexity of the movement, in order to improve anchorage, point of application and direction of force. However, in 2016, Align Technology introduced Invisalign®'s "G6 protocol" to enhance the results of closing spaces in cases of first premolar extractions; and through the use of the SmartForce® function (attachments optimized for canine retraction and maximum molar anchorage), SmartStage® technology (avoids anterior tilting and extrusion), and the use of devices power arms, improved predictability and outcomes in cases of extractions and maximum anchorage [14].
Success Rate in Percentage of Space Closure
The success rate of closing spaces was reported by only one publication (n=1). Gu, et al. (2017) [5] They mentioned that the average accuracy of tooth movement with Invisalign® was around 41%, and that between 70-80% of orthodontists required mid-process correction, refinement or conversion to fixed arch appliances to complete the treatment. They also reported that the overall average efficiency of tooth movement is 59% [5].
Effects on Gingival Architecture, After the Closure of Spaces
Only two of the articles in the final filter (16.67%) mention the effects generated on gingival architecture. Madariaga et al. (2020) [18] they determined that patients with aligners had less bleeding on probing but a greater number of recessions compared to those under orthodontic treatment with the arch technique (p=0.016); This may be due to the expansion of the arch during treatment and the difference in age between the groups studied, with the difference in the aligner group being greater. However, there was no difference in the periodontal health of patients undergoing fixed orthodontic therapy and aligner therapy, when establishing a program with regular controls and adequate oral hygiene instructions. Rather, Miethke et al. (2007) [13] reported that patients undergoing orthodontic treatment with aligners had a significantly lower depth of the groove at probing (p less than 0.01).
Other findings
Unwanted movements or side effects of closure (uncontrolled tilt, absence of 100% space, rotations, changes in the occlusal plane, others):
28.5% (n=4) evaluated unwanted movements during treatment. Hennessy et al. (2016) [15] they described that 71% of patients with Invisalign® had lower incisor proinclination, with an average of 3.4o±3.2o; however, it is a statistically and clinically non-significant difference compared to the group treated with the arch technique (p>0.05). In addition, Koumpia et al. (2008) [23] found a statistically significant difference in the OGS score between both groups: Invisalign® 22.3±8.7 and edge arch technique 29.9±9.3 (p=0.046).
On the other hand, Lin et al. (2021) [17] assessed occlusal contacts post-treatment (T1) and after 6 months of retention (T2) using ABO Objective Rating System (OGS) scores. Regarding occlusal contacts at T1, a score of 1 (occlusal discrepancies less than1) was determined for the Invisalign® group and 2 (occlusal discrepancies >1) for the fixed arch of ridge appliances group; and at T2, a score of 0 (satisfactory) was found for the Invisalign® group and 1 for the fixed appliance group. However, the results were not statistically significant at T1 (p=0.532) or T2 (p=0.373).
Pain Perception
Three of the selected articles make reference to the perception of pain by comparing the two techniques; of which, all They mentioned that the pain is less with the aligners [14,16,20]. Agarwal et al. (2021) [16] reported that the average pain/discomfort was significantly lower in the aligner group. Likewise, Antonio, et al. (2019) [14] they found that, according to the VAS (Visual Analog Scale used to catalog pain), from 4 hours until after the seventh day, pain with Invisalign® was always lower than in the opposite. In addition, Alcón et al. (2022) [20] they established that, according to the VAS, in the first month of treatment, the Invisalign® group presented less pain. However, they mention that from the second month and until the end of treatment (month 12), the level of pain is higher in the Invisalign® group.
Discussion
The present study sought to identify whether the aligner technique is as effective as the arch orthodontic technique for the closure of interdental spaces in individuals with permanent dentition under orthodontic treatment. The results showed that both techniques are effective, in terms of reducing the space in millimeters, and that the predominant type of movement with aligners during this closure is the progressive inclination in small increments, achieving an adequate root angulation adjacent to the space.
As for Reduction of space in millimeters, when comparing both techniques, statistically significant differences were found in this review, with reference to the interproximal contact score according to the OGS and the alignment scores of the anterior segment (maxillary and mandible), according to the post-treatment PAR Index, achieving from a residual space of 1 mm to complete closure of the space. This is consistent with the findings of Jaber et al. (2022) [24] who evaluated cases of extractions of first premolars, finding that for the alignment of the anterior maxillary and mandibular segment after treatment, the in-house aligner group had a score of 0.44±1.87 and 0.83±0.98 respectively, and the arch orthodontics group was 0.05±0.23 and 0.22±0.54 respectively, with no statistically significant differences for both categories.
Djeu et al. (2005) [19]; They found that the aligners can produce adequate gap closure, up to 6 mm in total; in line with what was proposed by Weir et al. (2016) [25] and Feng et al. (2022) [26], who demonstrated that the complete reduction in millimeters of the same was achieved. In contrast, with regard to arch orthodontics, no article was specific on the subject. However, authors such as Nightingale et al. (2003) [27] and Dixon et al. (2002) [28] show that the complete closure of the space was achieved, but Jacobs et al. (2011) [29], in their study of extractions of first molars, reported that a residual space remains.
In this review, it was found that the total treatment time was shorter in patients with aligners compared to the arch technique of edge; and, specifically, in patients with extractions under treatment with Invisalign®, one of the authors reported that the duration of treatment is 44% longer than treatment with fixed appliances; which coincides with what was reported by Papadimitriou et al. (2018). On the contrary, in an article comparing the closing time of premolar extractions with both techniques, Jaber et al. (2022) [24] report that the duration of treatment with in-house aligners is 23.27±5.28 months, while with conventional orthodontics it is 26.20±5.27 months, with no statistically significant difference (p=0.123).
On the other hand, although the approximate period of treatment with aligners is 11.5-19.52 months, it varies when it comes to the closure of spaces. Regarding premolar extractions, Dai et al. (2019) [11] They mention that, in cases of extractions of upper first premolars, it is 22.3±4.6 months. Later, Dai et al (2021) [8] indicate that in cases of extractions of 4 first premolars, The average time to close spaces is 21±4.2 months. For their part, Greco et al. (2021) [30] report that, thanks to a personalized digital treatment plan, and the application of the Invisalign® G6 protocol, the closure of extraction space is achieved in 15 months with an acceptable root parallelism. Likewise, in cases of removal of a lower incisor, Weir (2016) [25] establishes that the average treatment time was 42 weeks, that is, 9.6 months; however, 50% of cases required a short refinement period with an average of six weeks. In another article, Boyd et al (2002) [31], report that in a case of multiple upper and lower diastema, the closure of spaces was achieved in 9 months. Regarding the total treatment time, with arch orthodontics, although the approximate period is 17-23.62 months, a publication was also identified that mentions the time in months, of the closure of specific spaces. In the case of space closure of an upper central incisor, Czochrowska et al. (2003) [32] they mention that the average time increases to 34 months.
The results reported by different authors are dissimilar and difficult to standardize in order to establish whether or not the duration of treatment with space closure is attributable to the technique per se.
This research suggests that the predominant type of movement during the closure of spaces, using the aligner technique, is the progressive inclination in small increments of the adjacent teeth, towards the space in question. In contrast, Dai et al. (2019) [11] They indicate that the use of aligners in patients with extractions is a challenge since they are not rigid enough to retain their original shape when closing the space. This can cause the crown of the posterior teeth to tilt mesially toward the extraction space, causing a distal tilt of the canines; which reduces the extraction space, generates loss of anchorage, lack of root parallelism and increases the difficulties of treatment. However, Feng et al. (2022) [33] They suggest that in order to maintain the dental inclination prior to the extraction of first premolars and avoid an unwanted inclination towards the extraction space, an anti-tipping design of canines and posterior teeth is needed; this is consistent with what was reported by Ren et al. (2022).
Zhu et al. (2023) [34], they mention in their finite element analysis, that closing spaces with aligners can be effective if the movements are planned understanding the moments and forces that are generated by the "compression" of the aligner on the teeth adjacent to the space. The three possible anchor groups when planning a closure of extraction spaces imply diverse biomechanical effects on both the anterior and posterior sectors, which makes it necessary to consider overcorrection, and/or additional compensatory forces (power arms, skeletal anchors or elastics) to achieve an effective closure. However, it seems that cases of moderate anchorage, or major forces with skeletal anchorage, show more stable force systems with predictable results.
Additionally, the evidence mentions that, when performing space closure in conventional orthodontics, two main groups of mechanics stand out. The first group corresponds to friction mechanics, which use auxiliary devices such as elastomeric chains or springs. The second group refers to frictionless mechanics, in which elements such as T-shaped lenses are used to close the space. However, Ribeiro et al. (2016) [35] They reported that in both mechanics the predominant type of movement during the closure of spaces involves the retroinclination and extrusion of the incisors because the force applied in these cases usually passes below the center of resistance of the anterior segment; which results in a clockwise moment that generates this effect.
Regarding the success rate of closing spaces, from this review, Gu et al. (2017) [5] they mention that the average accuracy of tooth movement with Invisalign® is around 41% and that the overall average efficiency of tooth movement is 59%.
This coincides with what was reported by Feng et al. (2022) [26], who refer to the fact that, with the use of aligners, the designed tooth movement cannot be completely achieved, ranging from 28-88% of the planned position depending on the teeth and the designed tooth movements. Likewise, Haouili et al. (2022) [12], show that the average accuracy of Invisalign® for all tooth movements was 50% [12]. In the light of the available evidence, it does not seem possible to identify whether the closure of a planned space is influenced by the initial dental position and by the infinite combination of malpositions that can be found, or by the sequential planning of the movements known as staging, as it could affect the tilting conditions of the teeth adjacent to the space.
On the other hand, this research shows that there are no significant differences in terms of the effects on gingival architecture, after the closure of spaces, when comparing both techniques. Authors such as Lanteri et al. (2018) [6], showed that there are no significant differences in the presence of new recessions for both groups.
Other Findings
When talking about secondary movements during aligner treatment, this review concludes that 71% of patients with Invisalign® have lower incisor proinclination; however, it does not represent a clinically significant difference compared to the opposite group [15]. However, most of the reports analyzed involve treatments without extractions. In contrast to our findings, authors such as Boyd et al. (2008) [36] indicate that an intrusion of 0.25-0.5 mm of the posterior sectors may occur due to the covering of the occlusal faces; which is solved during the retention phase, thanks to the passive eruption of these segments until an adequate occlusal coupling is achieved. Also, Greco at al. (2021) [30], indicate that during the closure of spaces with aligners, loss of anterior torque, distal inclination of the canines and mesial inclination of the posterior sector due to the loss of anchorage may occur.
Additionally, Zhu et al. (2023) [34] they determined that direct anchoring during the closure of spaces with aligners reduced the rotation of the occlusal plane in a clockwise direction; while indirect anchoring was conducive to controlling the inclination of the anterior teeth. Thus, when using direct anchoring, an increase in the retraction force would require a more specific overcorrection of the anterior teeth to resist tilting; Mainly including lingual root control of the central incisor, followed by control of the distal root of the canine, control of the lingual root of the lateral incisor, control of the distal root of the lateral incisor, and control of the distal root of the central incisor. However, the retraction force could not eliminate the mesialization of the posterior teeth, causing a reciprocal closure, which could be used in favor in cases that do not require maximum anchorage.
In relation to pain perception, this review reported that pain was lower with aligners. According to the VAS, during the first month of treatment, there was less perception of pain with aligners compared to arch orthodontics; while from the second month to the 12th month, the level of pain is higher with aligners [14,20]. However, it is important to mention that we did not find articles that analyzed the perception of pain, in the specific context of closing spaces with aligners.
On the other hand, specifically in the closure of spaces with an arch of edge, a study evaluated pain according to VAS, in two groups, of which, one underwent the extraction of premolars only and the other group had mini-screws placed for the closure of spaces [37]. Significantly lower pain levels (p less than 0.001) were found in this study after the placement of mini-screws in comparison with premolar extractions both at night and 1 week after the procedure [37].
Conclusions
Recent developments in the area of research have led to innovations in aligner treatment, expanding their application from patients who do not require complex mechanics to those who even require the closure of spaces after extractions.
- Regarding the reduction of the space in millimeters, both techniques were shown to be equally effective, achieving a residual space of 1 mm until complete closure.
- With reference to the behavior of time in months, for the closure of spaces, the total duration of treatment is shorter with aligners. However, the results are dissimilar and difficult to standardize in order to verify whether or not the duration of treatment with space closure is attributable to the technique or the complexity of the case.
- During the closure of spaces with the arch ridge orthodontic technique, there is a coronal tilting movement of the adjacent teeth towards the edentulous space; whereas, when using aligners, the closure is carried out by progressively tilting the teeth adjacent to the edentulous space in small increments.
- Regarding the success rate in percentage for the closure of spaces, it was established that the average accuracy of tooth movement in general, with Invisalign® was around 41% and the average overall efficiency of tooth movement was 59%.
- There are no significant differences in terms of the effects on gingival architecture, after the closure of spaces, when comparing both techniques.
- The secondary occlusal effect, derived from the closure of spaces more prevalent in both techniques, involves the retroinclination of the anterior segment.
- It was reported that the pain is less with the aligners. Specifically, pain perception during the first month of treatment was lower with aligners, but it was higher from the second month to one year (calculated using VAS).
The literature recovered in this review showed that the closure of spaces with aligners is as effective as that performed using the arch technique of edge; however, it was not possible to identify scientific evidence, with the required methodological quality, to establish concrete differences in the different aspects related to the closure of spaces by comparing the two techniques.
Limitations
Within the limitations of this systematic review, it is evident that most of the studies identified did not include the closure of spaces, directly comparing both techniques, as the main objective; therefore, it was not possible to identify a high level of evidence to respond to the objectives initially set. In addition, the breadth of the search was limited by setting very specific objectives, which reduced the amount of literature available to respond to the established approach. Finally, a significant number of studies were excluded due to the type of design, the outcome, the object of study and for not meeting the methodological quality criteria.
Recommendations
It is recommended to continue the development of research, mainly randomized controlled clinical trials, to establish the effectiveness in the closure of spaces with aligners and with arch orthodontics; comparing both techniques in the same study in order to analyze the relationship between them. Additionally, studies are required that describe: the time of closure of spaces in months, the success rate in percentage of closure, the predominant movement of the teeth for closure in both techniques to obtain results that allow to be safely extrapolated to the clinic.
Declarations
Conflicts of Interest
The authors state that there were no conflicts of interest in the research.
Funding
This research did not receive any external funding.
Annex 1
References
- Ho, C. T., Huang, Y. T., Chao, C. W., Huang, T. H., Kao, C. T. (2021). Effects of Different Aligner Materials and Attachments on Orthodontic Behavior. Journal of Dental Sciences, 16(3):1001-1009.
Publisher | Google Scholor - Giancotti, A., Greco, M., Mampieri, G. (2006). Extraction Treatment Using Invisalign Technique. Prog Orthod, 7(1):32-43.
Publisher | Google Scholor - Jiang, T., Wu, R. Y., Wang, J. K., Wang, H. H., Tang, G. H. (2020). Clear Aligners for Maxillary Anterior En Masse Retraction: A 3D Finite Element Study. Scientific Reports, 10(1):10156.
Publisher | Google Scholor - Miller, D. B. (2009). Invisalign in TMD Treatment. International Journal of Orthodontics (Milwaukee, Wis.), 20(3):15-19.
Publisher | Google Scholor - Gu, J., Tang, J. S., Skulski, B., Fields Jr, H. W., Beck, F. M., et al. (2017). Evaluation of Invisalign Treatment Effectiveness and Efficiency Compared with Conventional Fixed Appliances Using the Peer Assessment Rating Index. American Journal of Orthodontics and Dentofacial Orthopedics, 151(2):259-266.
Publisher | Google Scholor - Lanteri, V., Farronato, G., Lanteri, C., Caravita, R., Cossellu, G. (2018). The Efficacy of Orthodontic Treatments for Anterior Crowding with Invisalign Compared with Fixed Appliances Using the Peer Assessment Rating Index. Quintessence International, 49(7).
Publisher | Google Scholor - Gaffuri, F., Cossellu, G., Lanteri, V., Brotto, E., Farronato, M. (2020). Comparative Effectiveness of Invisalign and Fixed Appliances in First-Premolar Extraction Cases. Journal of Clinical Orthodontics, 54(5):294-301.
Publisher | Google Scholor - Dai, F. F., Xu, T. M., Shu, G. (2021). Comparison of Achieved and Predicted Crown Movement in Adults After 4 First Premolar Extraction Treatment with Invisalign. American Journal of Orthodontics and Dentofacial Orthopedics, 160(6):805-813.
Publisher | Google Scholor - Simon, M., Keilig, L., Schwarze, J., Jung, B. A., Bourauel, C. (2014). Forces and Moments Generated by Removable Thermoplastic Aligners: Incisor Torque, Premolar Derotation, and Molar Distalization. American Journal of Orthodontics and Dentofacial Orthopedics, 145(6):728-736.
Publisher | Google Scholor - Ravera, S., Castroflorio, T., Garino, F., Daher, S., Cugliari, G., et al. (2016). Maxillary Molar Distalization with Aligners in Adult Patients: A Multicenter Retrospective Study. Progress in Orthodontics, 17(1):12.
Publisher | Google Scholor - Dai, F. F., Xu, T. M., Shu, G. (2019). Comparison of Achieved and Predicted Tooth Movement of Maxillary First Molars and Central Incisors: First Premolar Extraction Treatment with Invisalign. The Angle Orthodontist, 89(5):679-687.
Publisher | Google Scholor - Haouili, N., Kravitz, N. D., Vaid, N. R., Ferguson, D. J., Makki, L. (2020). Has Invisalign Improved? A Prospective Follow-Up Study on The Efficacy of Tooth Movement with Invisalign. American Journal of Orthodontics and Dentofacial Orthopedics, 158(3):420-425.
Publisher | Google Scholor - Miethke, R. R., Brauner, K. (2007). A Comparison of The Periodontal Health of Patients During Treatment with The Invisalign® System and with Fixed Lingual Appliances. Journal of Orofacial Orthopedics/Fortschritte der Kieferorthopädie, 68(3):223-231.
Publisher | Google Scholor - Antonio Zancajo, L. (2019). Estudio comparativo del dolor orofacial utilizando diferentes técnicas de ortodoncia: lingual, vestibular y alineadores (Invisalign®).
Publisher | Google Scholor - Hennessy, J., Garvey, T., Al-Awadhi, E. A. (2016). A Randomized Clinical Trial Comparing Mandibular Incisor Proclination Produced by Fixed Labial Appliances and Clear Aligners. The Angle Orthodontist, 86(5):706-712.
Publisher | Google Scholor - Agarwal, S. S., Datana, S., Kumar, M. P., Sharma, M., Andhare, P. (2023). Comparison of Efficacy Between MBT Preadjusted Edgewise Appliance and Clear Aligner Therapy Among Class I Crowding Cases: A Randomized Controlled Trial. Medical Journal Armed Forces India, 79:S54-S62.
Publisher | Google Scholor - Lin, E., Julien, K., Kesterke, M., Buschang, P. H. (2022). Differences in Finished Case Quality Between Invisalign and Traditional Fixed Appliances. The Angle Orthodontist, 92(2):173-179.
Publisher | Google Scholor - Pango Madariaga, A. C., Bucci, R., Rongo, R., Simeon, V., D’Antò, V., et al. (2020). Impact of Fixed Orthodontic Appliance and Clear Aligners on The Periodontal Health: A Prospective Clinical Study. Dentistry Journal, 8(1):4.
Publisher | Google Scholor - Djeu, G., Shelton, C., Maganzini, A. (2005). Outcome Assessment of Invisalign and Traditional Orthodontic Treatment Compared with The American Board of Orthodontics Objective Grading System. American Journal of Orthodontics and Dentofacial Orthopedics, 128(3):292-298.
Publisher | Google Scholor - Alcón Vidal, S. (2022). Dolor y calidad de vida en pacientes portadores de ortodoncia con alineadores (Invisalign) versus aparatología fija multibrackets: estudio clínico longitudinal.
Publisher | Google Scholor - Christou, T., Abarca, R., Christou, V., Kau, C. H. (2020). Smile Outcome Comparison of Invisalign and Traditional Fixed-Appliance Treatment: A Case-Control Study. American Journal of Orthodontics and Dentofacial Orthopedics, 157(3):357-364.
Publisher | Google Scholor - Buschang, P. H., Shaw, S. G., Ross, M., Crosby, D., Campbell, P. M. (2014). Comparative Time Efficiency of Aligner Therapy and Conventional Edgewise Braces. The Angle Orthodontist, 84(3):391-396.
Publisher | Google Scholor - Koumpia, E., Karagiannis, V., Tuncay, O. C. (2008). Case Series Report of Clear Aligner and Low-Friction Self-Ligating Brackets. Hellenic Orthodontic Review, 11(2).
Publisher | Google Scholor - Jaber, S. T., Hajeer, M. Y., Burhan, A. S., Hajeer, M. Y. (2022). The Effectiveness of In-House Clear Aligners and Traditional Fixed Appliances in Achieving Good Occlusion in Complex Orthodontic Cases: A Randomized Control Clinical Trial. Cureus, 14(10).
Publisher | Google Scholor - Weir, T. (2016). Invisalign Treatment of Lower Incisor Extraction Cases. Australian Orthodontic Journal, 32(1):82-87.
Publisher | Google Scholor - Feng, X., Jiang, Y., Zhu, Y., Hu, L., Wang, J., et al. (2022). Comparison Between the Designed and Achieved Mesiodistal Angulation of Maxillary Canines and Posterior Teeth and Influencing Factors: First Premolar Extraction Treatment with Clear Aligners. American Journal of Orthodontics and Dentofacial Orthopedics, 162(2):e63-e70.
Publisher | Google Scholor - Nightingale, C., Jones, S. P. (2003). A Clinical Investigation of Force Delivery Systems for Orthodontic Space Closure. Journal of Orthodontics, 30(3):229-236.
Publisher | Google Scholor - Dixon, V., Read, M. J. F., O'brien, K. D., Worthington, H. V., Mandall, N. A. (2002). A Randomized Clinical Trial to Compare Three Methods of Orthodontic Space Closure. Journal of Orthodontics, 29(1):31-36.
Publisher | Google Scholor - Jacobs, C., Jacobs-Müller, C., Luley, C., Erbe, C., Wehrbein, H. (2011). Orthodontic Space Closure After First Molar Extraction Without Skeletal Anchorage. Journal of Orofacial Orthopedics/Fortschritte der Kieferorthopädie, 72(1):51-60.
Publisher | Google Scholor - Greco, M., Pedernera, M. (2021). Tratamiento de clases II con extracciones y alineadores. Ortodoncia española: Boletín de la Sociedad Española de Ortodoncia, 1:105-119.
Publisher | Google Scholor - Boyd, R. L., Miller, R. J., Vlaskalic, V. (2000). The Invisalign System in Adult Orthodontics: Mild Crowding and Space Closure Cases. Journal of Clinical Orthodontics, 34(4):203-212.
Publisher | Google Scholor - Czochrowska, E. M., Skaare, A. B., Stenvik, A., Zachrisson, B. U. (2003). Outcome of Orthodontic Space Closure with A Missing Maxillary Central Incisor. American Journal of Orthodontics and Dentofacial Orthopedics, 123(6):597-603.
Publisher | Google Scholor - Feng, X., Jiang, Y., Zhu, Y., Hu, L., Wang, J., et al. (2022). Comparison Between the Designed and Achieved Mesiodistal Angulation of Maxillary Canines and Posterior Teeth and Influencing Factors: First Premolar Extraction Treatment with Clear Aligners. American Journal of Orthodontics and Dentofacial Orthopedics, 162(2):e63-e70.
Publisher | Google Scholor - Zhu, G. Y., Zhang, B., Yao, K., Lu, W. X., Peng, J. J., et al. (2023). Finite Element Analysis of The Biomechanical Effect of Clear Aligners in Extraction Space Closure Under Different Anchorage Controls. American Journal of Orthodontics and Dentofacial Orthopedics, 163(5):628-644.
Publisher | Google Scholor - Ribeiro, G. L. U., Jacob, H. B. (2016). Understanding The Basis of Space Closure in Orthodontics for A More Efficient Orthodontic Treatment. Dental Press Journal of Orthodontics, 21:115-125.
Publisher | Google Scholor - Boyd, R. L. (2008). Esthetic orthodontic treatment using the invisalign appliance for moderate to complex malocclusions. Journal of Dental Education, 72(8):948-967.
Publisher | Google Scholor - Ganzer, N., Feldmann, I., Bondemark, L. (2016). Pain and Discomfort Following Insertion of Miniscrews and Premolar Extractions: A Randomized Controlled Trial. The Angle Orthodontist, 86(6):891-899.
Publisher | Google Scholor























