

Clinical Trial
Diagnostic Triads in Cranial Base Tumors
Hermanos Ameijeiras Hospital. Neurosurgery Service. Havana, Cuba.
*Corresponding Author: Carlos Roberto Vargas Gálvez, Hermanos Ameijeiras Hospital. Neurosurgery Service. Havana, Cuba.
Citation: Omar L. Arbolay, Machín M.M.O., Gálvez C.R.V. (2026). Diagnostic Triads in Cranial Base Tumors. Journal of Neuroscience and Neurological Research. BioRes Scientia Publishers. 5(1):1-8. DOI: 10.59657/2837-4843.brs.26.033
Copyright: © 2026 Carlos Roberto Vargas Gálvez, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: May 08, 2025 | Accepted: January 12, 2026 | Published: January 19, 2026
Abstract
Introduction: Cranial base tumors constitute a wide variety of common lesions of the central nervous system. From a clinical perspective, they are characterized by nonspecific symptoms and signs. On the other hand, imaging studies provide morphological and extension characteristics in this region. The association between clinical and imaging elements through the formation of a diagnostic triad that allows us to associate with high certainty a histopathological variant and thus a better treatment.
Objective: Describe diagnostic triads associated with cranial base tumors.
Method: A descriptive, retrospective and observational study was carried out that included 808 patients from the “Hermanos Ameijeiras” Hospital operated on for cranial base tumors by endoscopic endonasal procedures. According to the histopathological variant in the cranial base, a diagnostic triad was formed for each tumor variant, composed of two clinical aspects and one imaging aspect.
Results: A high correspondence of the diagnostic triad with a histopathological variant was generally evident. The diagnostic triad of pituitary adenomas (96.7 %) is reported most frequently, followed by the triad of craniopharyngiomas (95.2 %) and clivus chordomas (95.0 %).
Conclusions: The study shows a high correspondence of diagnostic triads with their respective cranial base tumors, which allows a better diagnostic and treatment process with patients.
Keywords: clinical diagnosis; diagnostic imaging; skull base; neoplasms of the central nervous system
Introduction
The history of medicine dates back thousands of years to ancient civilizations that developed medical knowledge and practices [1]. Over time, medicine has evolved and transformed into a scientific and professional discipline [2]
When faced with an illness or disease, it is essential to make an early and accurate diagnosis to establish an accurate treatment. Without a wise diagnosis, treatment can be ineffective or even harmful, which is why it is essential to identify a disease, interfere with and modify its evolution, prognosis and reduce its complications [3].
In the practice of medicine, despite the notable technological advances today, clinical and surgical practice continues to be based on inviolable basic pillars that include: the patient's personal history, the questioning of the disease, history of the disease, the examination physical and the diagnostic hypothesis is confirmed with diagnostic studies (hematological, microbiological, histopathological and imaging).
In the 5th century BC, Hippocrates, [4] the father of medicine and one of the pioneers in assigning symptoms and signs associated with a certain disease, described the called Hippocrates triad that includes: abdominal pain, abdominal distension and sensitivity to pressure for what is currently known as peritonitis.
The word triad comes from the Greek triás, which means set of three [5]. In medicine, a diagnostic triad represents a set of 3 linked elements that guide the diagnosis of a disease.
In this sense, in the study of the central nervous system, today various diagnostic triads are described, which allow the practice of personalized medicine, with greater effectiveness and among these the following stand out:
Table 1: Diagnostic triads described in the central nervous system
| Triad | Elements of the triad |
| Hakim-Adams Triad [6] (hydrocephalus of the elderly) | Dementia, urinary incontinence and gait apraxia. |
| Cushing's triad [7] (intracranial hypertension) | Intracranial hypertension, bradycardia and irregular breathing. |
| Triad in Gillain Barré [8] (autoimmune disease that affects the nervous system) | Areflexia, ascending weakness, paresthesias in hands and feet. |
| Virchow Triad [9] (cerebral vein thrombosis) | Venous congestion, cerebral edema and intracerebral hemorrhage |
| Dandy-Walker Triad[10] (posterior fossa malformation) | Partial or complete agenesis of the vermis, cystic dilation of the fourth ventricle and elongation of the posterior fossa. |
| Charcot triad [11] (multiple sclerosis) | Nystagmus, ataxia and dysarthria. |
| Meniere's triad [12] (inner ear abnormality) | Tinnitus, vertigo, hearing loss |
| Susac Triad [14] (microangiopathy of the brain, retina and cochlea) | Encephalopathy, visual disturbances and hearing loss |
| Horner's triad [15] (oculosympathetic pathway injury) | Anisocoria, ptosis, hemifacial anhidrosis. |
| Parkinson's triad [16] (Parkinson's disease) | Akinesia, tremor at rest, rigidity. |
| West Triad [16] (epileptic encephalopathy) | Hypsarrhythmia, mental retardation, infantile spasms. |
The systematic and critical review of epidemiological studies worldwide describe that the prevalence of these tumors varies between 30.0 - 40.0% of tumors of the central nervous system [17-19]. In this sense, various variants of tumors in the cranial base are described, which in their genesis develop at the expense of neurovascular structures (dura mater, nerves, pituitary gland, bone, among others) [17]. On the other hand, they are characterized by manifestations great variety of symptoms and signs, as well as a wide diversity of imaging aspects (table 2).
Table 2: Characteristics according to type of histopathological variant, anatomical origin in the cranial base, main clinical and imaging manifestations.
| Histopathological variant | Anatomical origin | Main clinical manifestations | Main imaging characteristics |
| Olfactory groove meningioma [20] | Cribriform plate or frontosphenoidal Suture | Anosmia, seizures, cognitive dysfunction. | Main imaging characteristics Image with defined borders in the fronto-basal region, tail or dural enhancement, hyperostosis in the adjacent bone. |
| Sellar tubercle meningioma [21] | Sphenoidal plane, sellar tubercle, chiasmatic groove, sphenoidal limbus and sellar diaphragm | Headache, visual disturbances, endocrine disorders | Image with defined borders in the region of the sellar tubercle, tail or dural enhancement, hyperostosis in the adjacent bone |
| Pituitary macroadenoma [22] | Adenohypophysis | Headache, ophthalmological (visual field defects) and endocrinological disorders | Rounded or lobed image that may be confined within the sella turcica or have supra or parasellar growth |
| Craniopharyngioma [23] | Pituitary stalk | Headache, ophthalmological, endocrinological and neurological disorders | Suprasellar image with mixed densities, presence of calcifications |
| Clivus chordoma [24] | Remnant undifferentiated cells of the notochord in the clivus | Occipital headache, swallowing difficulties, facial muscle weakness, voice changes, balance and coordination problems, and cranial nerve dysfunction, double vision or visual field defects | Mass lesion in the region of the clivus, with its destruction and extension to the nasopharynx, with calcifications |
| Petroclival meningioma [25] | Medial and dorsal to the clivus | Cranial nerve dysfunction, swallowing disorders, voice changes, dizziness, imbalance and incoordination, facial pain, visual disorders (diplopia and visual field defects) | Image in relation to the brain stem, vessels and cranial nerves, compression or displacement of neurovascular structures of the posterior fossa |
| Cerebellopontine angle meningioma [26] | Angle formed between the cerebellum and the brain stem, specifically in the region of the temporal bone | Unilateral or bilateral hearing loss, tinnitus and sensation of fullness in the ear, dizziness, vertigo, unsteadiness when walking, imbalance, facial paralysis | Image with defined borders in the cerebellopontine angle, tail or dural enhancement; adjacent hyperostosis |
| Cranio-spinal junction meningioma [27] | Arachnoids surrounding the foramen magnum and axial cervical portion (up to the second cervical vertebra) | Occipital or cervical pain, pain in the extremities, paresthesias, muscle weakness, urinary or fecal incontinence. | Image with defined borders between the foramen magnum and the second cervical vertebra in its anterior or posterior portion, tail or dural enhancement, hyperostosis in the adjacent bone |
Preoperative diagnosis of the histopathological variant of these complex tumors is essential for effective treatment options. The objective of the present investigation is to describe the association of clinical and imaging manifestations formed by a diagnostic triad that associates with tumors of the cranial base for a more effective diagnosis and treatment.
Methods
A retrospective descriptive study was carried out, between January 2015 and December 2023, in 843 patients with various tumors of the cranial base with surgical criteria for endoscopic endonasal surgery and endoscopic keyhole approach to the cranial base at the Hermanos Ameijeiras University Hospital, in Havana (Cuba).
The database was obtained from the medical records system of the health facility during the time of the investigation.
Patients with clinical and imaging suspicion of a tumor in the cranial base, aged 19 years or older, with surgical criteria for these procedures, were taken into account as inclusion criteria. Patients with acute or chronic decompensated illnesses that made surgical treatment impossible were excluded.
For each histopathological variant, a diagnostic triad was formed, consisting of 2 clinical manifestations (symptoms or signs) and 1 imaging characteristic (according to brain magnetic resonance imaging (MRI).
In relation to the clinical elements, these were defined as the 2 most frequent clinical manifestations referred by patients or identified during the physical examination by health personnel.
While the imaging element using MRI was defined according to the most frequent tumor characteristic, in a particular manner according to the topography and possible tumor variant.
For data analysis, absolute and relative frequencies were used as summary measures. All hypothesis tests used were two-tailed. They were considered significant, with a bilateral p-value less than 0.05.
Variables to evaluate
• Histopathological variant: depending on the type of tumor at the cranial base.
• Diagnostic triad (table 3).
• Diagnostic triad: presence or absence.
Table 3: Clinical and imaging elements that conform the diagnostic triad according to tumor diagnosis.
| Tumor diagnosis | Clinical elements | Imaging element | Diagnostic triad |
| Olfactory Groove meningioma | Frontal headache and olfactory disorders | Extra axial image over the cribriform plate of the ethmoid | Frontal headache, olfactory disorders and extra-axial image on the cribriform plate of the ethmoid |
| Sellar tubercle meningioma | Retro-ocular headache and asymmetric campimetric visual defect | Image that rides on the sellar tubercle | Retro-ocular headache, asymmetric campimetric visual defect and image that rides on the sellar tubercle |
| Pituitary adenoma | Partial hypopituitarism and symmetric field visual defect | Image that deforms the sella turcica | Partial hypopituitarism, symmetrical campimetric visual defect and image that deforms the sella turcica |
| Craniopharyngioma | Pan hypopituitarism and symmetric field visual defect | Suprasellar image of mixed intensity that respects the sella turcica | Pan hypopituitarism, symmetrical campimetric visual defect and suprasellar image of mixed intensity that respects the sella turcica |
| Clivus chordoma | Suboccipital headache and seizure of the VI cranial nerve | Image with destruction of the clivus | Suboccipital headache, seizure of the VI cranial nerve and image that destroys the clivus |
| Petroclival meningioma | Occipital headache and seizure of the VI cranial nerve | Retroclival image that deforms the brain stem in the shape of an inverted comma | Headache, seizure of the VI cranial nerve and retroclival image that displaces the brain stem in the shape of an inverted coma |
| Cerebellopontine angle meningioma | Occipital headache and early seizure of the VII and/or late seizure of the VII cranial nerve | Image in the cerebellopontine angle that deforms the brain stem into a comma shape. | Occipital headache, capture of the VII and/or cranial nerve and image in the ponto-cerebellar angle that deforms the brain stem in the shape of a coma |
| Cranio-spinal junction meningioma | Suboccipital headache, seizure of lower cranial nerves (IX,X,XI) and/or asymmetric motor defect | Anterolateral extra-axial image that displaces the medullary-medullary junction | Suboccipital headache, seizure of lower cranial nerves (IX, X, XI) and/or asymmetric motor defect and image that displaces the medullary junction |
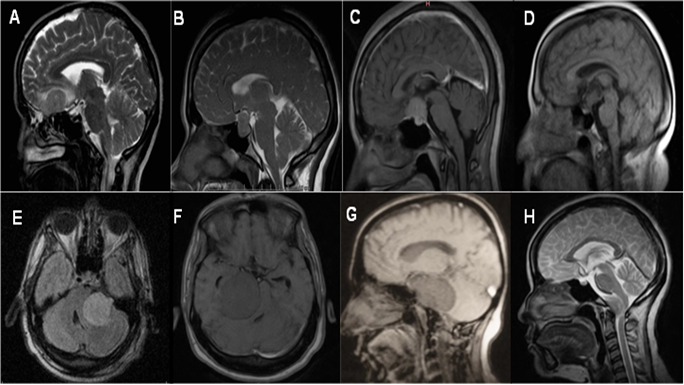
Figure 1: Imaging element that conforms the diagnostic triad are: A) Olfactory groove meningioma, extra-axial image on the cribriform plate of the ethmoid. B) Pituitary adenoma, image that deforms the sella turcica. C) Sellar tubercle menigioma, an image that rides on the sellar tubercle. D) Craniopharyngioma, suprasellar image of mixed intensity that respects the sella turcica. E) Petroclival meningioma, retroclival image that deforms the brain stem in the shape of an inverted comma. F) Cerebellopontine angle meningioma, an image in the cerebellopontine angle that deforms the brain stem in the shape of a comma. G) Chordoma of the clivus, image with destruction of the clivus. H) Cranio spinal junction meningioma, extra-axial anterolateral image, that displaces the medullary-medullary junction.
Ethical considerations
The conduct of this study was endorsed by the ethics committee and the scientific council of the “Hermanos Ameijeiras” Hospital. Participation was voluntary and certified through informed consent. The provisions established according to the current scientific research standards, emanating from the Declaration of Helsinki, were complied with.
Results
Table 4 shows the distribution of patients according to the analysis of the diagnostic triad and its histopathological variant. Overall, the diagnostic triads were present in more than 90% of the patients. Patients with pituitary adenomas were those with a greater presence of the diagnostic triad (96.7%), followed by craniopharyngiomas (95.2%) and clivus chordomas (95.0%). On the other hand, petroclival meningiomas were accompanied by a lower presence of the diagnostic triad (92.0%), followed by cerebellopontine angle meningioma (92.7%), and cranio-spinal junction meningioma (90.0%).
Table 4: Characteristics of patients with the diagnostic triad and histopathological diagnosis.
| Diagnosis | Diagnostic triad | Total |
p | ||||
| Presence | Absence | ||||||
| n | % | n | % | n | % | ||
| Pituitary adenomas | 584 | 96,7 | 20 | 3,3 | 604 | 71,2 | less than 0,0001 |
| Craniopharyngioma | 59 | 95,2 | 3 | 4,8 | 62 | 7,4 | less than 0,0001 |
| Sellar tubercle meningioma | 48 | 94,1 | 3 | 5,9 | 51 | 6,0 | less than 0,0001 |
| Cerebellopontine angle meningioma | 38 | 92,7 | 3 | 7,3 | 41 | 4,9 | less than 0,0001 |
| Olfactory groove meningioma | 28 | 93,3 | 2 | 6,7 | 30 | 3,6 | less than 0,0001 |
| Petroclival meningioma | 23 | 92,0 | 2 | 8,0 | 25 | 3,0 | less than 0,0001 |
| Clivus chordoma | 19 | 95,0 | 1 | 5,0 | 20 | 2,4 | less than 0,0001 |
| Cranio spinal junction meningioma | 9 | 90,0 | 1 | 10,0 | 10 | 1,2 | 0,002 |
| Total | 808 | 95,8 | 35 | 4,2 | 843 | 99,7 | less than 0,0001 |
Discussion
The practice of medicine includes applying in an ideal, timely and efficient manner the knowledge and resources that science and medical art offer in order for the patient to cope with their illness, whether restoring their health, preserving their life, alleviating their ailments, or recovering their state of health [1,2]. In this sense, accurate diagnostic thinking is essential, which guides an effective treatment process that includes the use of pharmacological, surgical and adjuvant measures (radiotherapy, chemotherapy, immunotherapy, radiosurgery, among others).
The nervous system, like a few organs, is characterized by a wealth of symptoms and signs, as well as by a diverse presence of imaging characteristics [19]. A fundamental pillar for an accurate diagnosis is clinical evaluation, which includes high skill, knowledge and expertise of health personnel. On the other hand, currently there is a wide presence of complementary studies that allow confirming the clinical diagnosis and include simple and contrasted tomography, simple and contrasted resonance, and angiography, among others [11-14].
Tumors of the cranial base occur with high frequency [19], the diagnosis is difficult due to the diversity of lesions in this region, an action that leads to the use of complex diagnostic studies, costly to the health system and even dangerous for patients. With a longer waiting time for treatment due to uncertainty in the diagnosis. However, the authors of this research provide clinical and imaging aspects grouped into diagnostic triads that lead to a diagnosis with high certainty, related to tumor genesis in the cranial base and its relationship with adjacent neuroanatomical structures.
In the CNS, the grouping of symptoms and signs formed into diagnostic triads for the treatment of various diseases has been historically reported [6-16]. However, little reference is made to tumors of the cranial base, most of these studies have focused on surgical results, [17-19] but not on diagnostic triads. The authors carried out an exhaustive collection of information in internet search engines: Scielo, SCOPUS, PUBMED, and Google Escholar and did not identify related diagnostic triads to cranial base tumors.
When analyzing tumors in the middle cranial fossa, 3 tumors stand out: pituitary adenomas, sellar tubercle meningiomas and craniopharyngiomas. Discerning between these 3 histopathological variants from a clinical and imaging perspective is a challenge due to the intimate relationship with the optic chiasm, the pituitary and the sellar region; [18,22] however, the grouping into diagnostic triads suggests aspects that make them unique and in the present study all triads were accompanied by high frequency and with statistical significance (table 4, p< 0>
In relation to pituitary adenomas, the diagnostic triad composed of partial hypopituitarism, symmetrical campimetric visual defect, and an image that deforms the sella turcica was the one that presented the greatest presence in the study. This is explained due to its genesis in the adenohypophysis, its compressive effect against the optic chiasm, and the morphological or destructive changes on the sella turcica [22].
When analyzing craniopharyngiomas, due to their origin in the pituitary stem, they present the triad composed of: pan hypopituitarism, due to its close relationship with the hypothalamic pituitary axis; symmetric campimetric visual defect, due to compression against the chiasm optical; and suprasellar image of mixed intensity that respects the sella turcica, given its cephalo posterior growth towards the pituitary stalk.
On the other hand, sellar tubercle meningioma are present in their triad: retro-ocular headache, asymmetric campimetric visual defect, and image that rides on the sellar tubercle, these elements as a result of tumor growth unilaterally in relation to the intracanalicular portion of the optic nerve.
The in-depth clinical analysis of the endocrinological manifestations suggests greater involvement in craniopharyngiomas, while the bilateral ophthalmological alteration is in adenomas and craniopharyngiomas; however, unilateral visual disorder is more common in sellar tubercle meningioma due to its origin and tumor growth in the optic sulcus, except in tumors of considerable size that contact both optic sulcus in which bilateral visual alterations can be seen, but in a manner. Initially the affectation is unilateral. From the imaging perspective (Figure 1), adenomas frequently alter the morphology of the sellar region by increasing width, length, or destroying the sella turcica; Craniopharyngiomas continue their growth in the pituitary stalk with their variations in intensity, whether mixed by solid, cystic or combined component; and sellar tubercle meningioma due to their position on the sellar tubercle.
In the anterior cranial fossa, the olfactory Groove meningioma stands out and the diagnostic triad was accompanied by frontal headache, olfactory disorders and extra-axial image on the cribriform plate of the ethmoid. Clinical and imaging characteristics with a high association with these tumors (table 4). These lesions are characterized by growth in the sphenoidal plane, sellar tubercle, chiasmatic groove, sphenoidal limbus and sellar diaphragm [20]. Frontal headache is due to the inflammatory response in the meninges, compression of neurovascular structures or due to increased intracranial pressure; while alterations in olfaction due to irritation or deterioration of the olfactory fillets in the anterior fossa, and from the imaging perspective (Figure 1) are characterized by a space occupying lesion in this topography in contact with the arachnoid.
For its part, the posterior cranial base is the largest of the 3 and houses critical neurovascular structures such as the brain stem, cranial nerves and basilar artery [19]. In this region, tumors such as cerebellopontine angle meningioma, petroclivals meningioma, and the cranio-spinal junction meningioma, as well as chordomas of the clivus, stand out [17,18].
The diagnostic triad of the cerebellopontine angle meningioma are made up of: occipital headache, a seizure of the VII cranial nerve, and image of the cerebellopontine angle that deforms the brain stem in the shape of a comma. These lesions grow in the virtual space formed between the cerebellum and the brain stem [18,19], in relation to the internal auditory canal, which is why there is alteration of the VII cranial nerve and the lateral displacement in the form of a coma in an imaging study (Figure 1).
Regarding petroclival meningiomas, they stand out for the triad consisting of an occipital headache, seizure of the VI cranial nerve, and retroclival image that displaces the brain stem in the shape of an inverted comma. A differential element is diplopia due to involvement of the VI cranial nerve, given by alterations in its path in the stem towards the posterior wall of the clivus and through the Dorello canal within the basilar venous plexus [25]. While the displacement of the brain stem is anteroposterior, it adopts the shape of an inverted comma.
When analyzing the cranio-spinal junction meningioma, they presented the triad composed of: suboccipital headache, seizure of lower cranial nerves IX; these are due to tumor growth in the arachnoid surrounding the foramen magnum in the anterior or posterior segment and axial cervical portion, the topography where the real origin of the IX, X, and XI nerves lies at the level of the medulla oblongata [25].
Regarding chordomas of the clivus, they are accompanied by the diagnostic triad composed of: suboccipital headache; a seizure of the VI cranial nerve, and image that destroys the clivus. This type of lesion differs from petroclival meningiomas in the imaging characteristics, specifically in that chordomas have an origin in the remaining cells of the notochord, they can present a variable behavior with aggressive characteristics with alterations at the level of the clivus, including its destruction [24].
The study shows a high correspondence of diagnostic triads with their respective cranial base tumors, which allows a better diagnostic and treatment process with patients.
Declarations
Conflicts of interest
The authors report no conflicts of interest.
Author contributions
Conceptualization: Omar López Arbolay, Marlon Manuel Ortiz Machín, Carlos Roberto Vargas Gálvez.
Data curation: Omar López Arbolay, Marlon Manuel Ortiz Machín, Carlos Roberto Vargas Gálvez.
Formal analysis: Omar López Arbolay, Marlon Manuel Ortiz Machín, Carlos Roberto Vargas Gálvez.
Research: Omar López Arbolay, Marlon Manuel Ortiz Machín, Carlos Roberto Vargas Gálvez.
Methodology: Omar López Arbolay, Marlon Manuel Ortiz Machín, Carlos Roberto Vargas Gálvez.
Project administration: Omar López Arbolay, Marlon Manuel Ortiz Machín, Carlos Roberto Vargas Gálvez.
Resources: Omar López Arbolay, Marlon Manuel Ortiz Machín, Carlos Roberto Vargas Gálvez.
Supervision: Omar López Arbolay, Marlon Manuel Ortiz Machín.
Validation: Omar López Arbolay, Marlon Manuel Ortiz Machín.
Visualization: Omar López Arbolay, Marlon Manuel Ortiz Machín, Carlos Roberto Vargas Gálvez.
Writing – original draft: Omar López Arbolay, Marlon Manuel Ortiz Machín, Carlos Roberto Vargas Gálvez.
Writing – review and editing: Omar López Arbolay, Marlon Manuel Ortiz Machín, Carlos Roberto Vargas Gálvez.
References
- Dobson J. (2019). The marvellous history of medicine. BMJ, 367:l6603.
Publisher | Google Scholor - Tybjerg K. (2022). Scale in the history of medicine. Stud Hist Philos Sci., 91:221-233.
Publisher | Google Scholor - Miziara ID, Miziara CSMG. (2022). Medical errors, medical negligence and defensive medicine: A narrative review. Clinics (Sao Paulo), 77:100053.
Publisher | Google Scholor - Benmoussa N, D'andrea G, Moya-Plana A, Philippe C. Hippocrates (2022). father of mini-invasive nasal surgery. Surg Radiol Anat., 44(10):1375-1378.
Publisher | Google Scholor - REAL ACADEMIA ESPAÑOLA. (2024). Dictionary of the Spanish language, 23rd edition
Publisher | Google Scholor - Keller NC, Schmid S, Hämmerle B (2020). Not every day Caused the Nocturia at dementia Development and Unsteady gait [ On Unusual Reason for Nocturia Combined with Cognitive Decline and Gait Disturbance]. Practice (Bern 1994). 109(15):1201-1204.
Publisher | Google Scholor - Auerbach M, Cole J, Violano P, Roney L, Doherty C, Shepherd M, et al. (2018) International Interprofessional Study of Mental Models and Factors Delaying Neuroimaging of Critically Head-Injured Children Presenting to Emergency Departments. Pediatr Emerg Care, 34(11):797-801.
Publisher | Google Scholor - Shahrizaila N, Lehmann HC, Kuwabara S. (2021). Guillain-Barré syndrome. Lancet, 397(10280):1214-1228
Publisher | Google Scholor - Lurie JM, Png CYM, Subramaniam S, Chen S, Chapman E, et al. (2019). Virchow's triad in silent deep vein thrombosis. J Vasc Surg Venous Lymphat Disord., 7(5):640-645.
Publisher | Google Scholor - Belser-Ehrlich J, Adrian Lafo J, Mangal P, Bradley M, Wicklund M, et al. (2020) Neurocognitive profile of a man with Dandy-Walker malformation: Evidence of subtle cerebellar cognitive affective syndrome. Clin Neuropsychol., 34(3):591-610.
Publisher | Google Scholor - Tan SY, Chong CF, Chong VH. (2020). Charcot's triad. QJM, 113(6):436
Publisher | Google Scholor - Chen JY, Guo ZQ, Wang J, Liu D, Tian E, et al., (2023). Vestibular migraine or Meniere's disease: a diagnostic dilemma. J Neurol., 270(4):1955-1968.
Publisher | Google Scholor - Marrodan M, Fiol MP, Correale J. Susac syndrome. (2022). challenges in the diagnosis and treatment. Brain, 145(3):858-871.
Publisher | Google Scholor - Bongomin F, Khan SA, Oravec T. (2020). A Complete Triad: Horner's Syndrome in Tuberculous Meningitis. Am J Med Sci., 360(2):204-205.
Publisher | Google Scholor - Béreau M, Castrioto A, Lhommée E, Maillet A, Gérazime A, et al., (2022). Fatigue in de novo Parkinson's Disease: Expanding the Neuropsychiatric Triad? J Parkinsons Dis., 12(4):1329-1337.
Publisher | Google Scholor - Pavone P, Polizzi A, Marino SD, Corsello G, Falsaperla R, et al. (2020). West syndrome: a comprehensive review. Neurol Sci., 41(12):3547–3562.
Publisher | Google Scholor - Forst DA, Jones PS. (2023). Skull Base Tumors. Continuum (Minneap Minn)., 29(6):1752–1778.
Publisher | Google Scholor - Zanoletti E, Mazzoni A, Martini A, Abbritti RV, Albertini R, et al. (2019). Surgery of the lateral skull base: a 50-year endeavor. Acta Otorhinolaryngol Ital., 39(SUPPL. 1) :S 1-S146.
Publisher | Google Scholor - Vargas Gálvez CR, López Arbolay O, Ortiz Machín MM. (2024). Minimally invasive approach for Skull -based meningiomas. Neurosurgery (Astur: Engl Ed)., 35(3):127–135.
Publisher | Google Scholor - Vargas Gálvez CR, López Arbolay O, Ortiz Machín MM. (2024). Cranial base reconstruction in patients with olfactory groove meningioma using endoscopic endonasal approaches. Rev Cuban Med Milit, 53(2).
Publisher | Google Scholor - López- Arbolay O, Ortiz-Machín M, Coronado-Rosales A, Menéndez-Palacios M, Solernou -Ferrer A. (2021). Meningiomas of the sellar tubercle. Considerations of the endoscopic endonasal approach. Annals of the Cuban Academy of Sciences, 11(2).
Publisher | Google Scholor - Tritos NA, Miller KK. (2023). Diagnosis and Management of Pituitary Adenomas: A Review . JAMA, 329(16):1386-1398.
Publisher | Google Scholor - Ortiz-Machín M, López- Arbolay O, Goyenechea-Gutiérrez F, Sánchez- Gendriz I. (2022). Extended endoscopic endonasal approach to craniopharyngiomas: the rule of 3 in surgical dissection. Annals of the Cuban Academy of Sciences, 12(3).
Publisher | Google Scholor - Gheorghiu ML, Gheorghisan-Galateanu AA. (2019). CLIVUS CHORDOMA. Acta Endocrinol (Buchar).,15(3):406.
Publisher | Google Scholor - Magill ST, McGahan BG, Carrau RL, Prevedello DM. (2022). Endoscopic endonasal transclival petroclival meningioma resection. Neurosurg Focus Video.,6(2):V 2.
Publisher | Google Scholor - Gezgin I, Yucetas C, Dogan A. (2023). Meningiomas of the Cerebellopontine Angle: Tips and Pearls for Safe Surgical Resection. Turk Neurosurg.,33(3):458-464.
Publisher | Google Scholor - Wang C, Zou Y, Zeng Q, Hong H, Zheng C. (2019). Isolated Rosai-Dorfman disease with craniocervical junction involvement in the foramen magnum: A case report. Medicine (Baltimore)., 98(40): e17433.
Publisher | Google Scholor























