

Research Article
Demand for Long-Acting Family Planning Methods and Associated Factors Among Family Planning Service Users in Public Health Centers, Debre Birhan, Ethiopia, 2025
- Aweke Ayalew *
- Melaku Derese
- Teshome Ayalew
- Berhanu Shetie
Debre Birhan University, Debre Berhan, Ethiopia.
*Corresponding Author: Aweke Ayalew, Debre Birhan University, Debre Berhan, Ethiopia.
Citation: Ayalew A, Derese M, Ayalew T, Shetie B. (2025). Demand for Long-Acting Family Planning Methods and Associated Factors Among Family Planning Service Users in Public Health Centers, Debre Birhan, Ethiopia, 2025, Clinical Case Reports and Studies, BioRes Scientia Publishers. 10(6):1-18. DOI: 10.59657/2837-2565.brs.25.276
Copyright: © 2025 Aweke Ayalew, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: September 09, 2025 | Accepted: September 23, 2025 | Published: September 30, 2025
Abstract
Background: Long-acting family planning methods are in high demand in order to improve reproductive health and lower the number of unwanted pregnancies. Even though long-acting family planning methods are quite effective, they are still not widely used, especially in low- and middle-income nations. Evidence indicates that the majority of women were dependent on short-acting contraceptive methods, despite the fact that long-acting methods are safer, more effective, and offer protection against unplanned pregnancy.
Objectives: The objectives of this study are to assess the demand of long-acting family planning methods and identify associated factors among family planning service users in Debre Birhane public health centers of Amhara region, Ethiopia 2025.
Methods: An institutional-based cross-sectional quantitative approach was conducted from February 1st to March 30th 2025. A sample size is 394 and systematic random sampling was employed for selecting study units. A pretested structured questionnaire was used to collected data from the study participants. For data entry KOBO tool box was used and transferred to SPSS version 27.0.1 for data process and analysis. Descriptive statistics used to describe study variables. Bivariate and multivariable regression analysis done with 95% confidence intervals and a p-value <0.05 considered to declare statistically significant associations lastly result presented using a text and table.
Result: The study included 390 respondents with 99% respondent rate. The demand for Long-acting family planning method was 100 (25.6%). Marital status, Multigravida, Information from mass media, good attitude on Long-acting family planning method, Age 35-49, education No formal education, age at marriage 25-35 and being student at high school and above and reproductive age group. Affect the demand for Long-acting family planning method in this study.
Conclusion: the demand for Long-acting family planning method according to this study was low and the unmet need for Long-acting family planning method also high. Marital status, Multigravida, Information from mass media, good attitude on Long-acting family planning method, Age 35-49, education No formal education, age at marriage 25-35 and being student at high school and above and reproductive age group. Affect the demand for Long-acting family planning method in this study.
Recommendation: Based on this study the demand for long-acting family planning method is low and unmet need for Long-acting family planning method was found high so it is better to utilize the opportunity to provide the service to meet.
Keywords: demand; long-acting family planning; reproductive age women; meet need; unmet need
Introduction: Background
A key element of reproductive health, family planning (FP) helps people and couples to plan for and achieve the number of children and spacing of births they wish [1]. It encompasses a range of practices and methods that allow people to make informed choices about their reproductive lives [2]. By giving people more control over their reproductive health, FP lowers the number of unwanted births, improves maternal and child health, and gives women the confidence to seek higher education and employment [3,4]. People utilize FP for numerous reasons, including the desire to limit family size, space births, and improve overall family well-being [5]. Effective family planning can lead to healthier pregnancies and births, as well as enhanced economic conditions for families by allowing parents to allocate resources more effectively [6]. Additionally, FP plays a crucial role in reducing maternal mortality rates, as it enables women to avoid high-risk pregnancies and childbirths [7]. The ability to plan and space pregnancies is particularly important in regions with high fertility rates, where access to FP services can significantly impact public health and socio-economic development [8].
The demand for effective FP methods is a critical aspect of reproductive health, particularly in low and middle-income countries (LMICs), where unintended pregnancies can have significant socio-economic consequences [9]. Among the various contraceptive options available, long-acting contraceptive methods (LACMs) such as intrauterine devices (IUDs) and hormonal implants stand out due to their high efficacy and convenience. Unlike short-acting methods, LACMs require minimal user intervention once administered, making them an appealing choice for many women seeking to prevent unintended pregnancies [3].
The demand for the use of LAFPMs is related to various factors. Therefore, it's critical to evaluate the demand for LAFPMs among FP service users in order to pinpoint different socio demographic, cultural, and health system elements. In the end, better family planning alternatives for women can result from comprehending and addressing the issues that affect the demand for LAFPMs. This will assist to lower the rates of unwanted births and improve general reproductive health.
Statement of The Problem
Despite their advantages, the uptake of Long-Acting family planning Methods remains low in worldwide. Every year approximately 350,000 women die while pregnant or giving birth, and of which 99% of women die in developing countries [10]. An estimated 8 million more women suffer serious illnesses and lifelong disability as a result of complication during childbirth. According to the World Health Organization (WHO), less than 10% of women in many LMICs use LAFPMs, compared to significantly higher rates in high-income countries [11]. Sub Saharan Africa countries faces serious population and reproductive health challenges, which is indicated by higher maternal mortality, higher total fertility and population growth rate, and higher unmet need for FP [12]. For instance, the unmet need of FP in LMICs range from 20% up to 58% [9]. In Ethiopia, from 871 per 100,000 live births in 2000 to 412 per 100,000 live births in 2016, Ethiopia's maternal mortality ratio has decreased. Ethiopia's maternal mortality ratio, according to the UN Interagency Maternal Mortality Ratio projection for 2020, is 267 per 100,000 live births, indicating considerable progress in reducing maternal mortality, however it is still far behind the SDG target of 70 [13]. The total fertility rate of Ethiopia is 5.4 children per women, population growth rate is estimated at 2.7% per year, contraceptive prevalence rate is only 15% and an unmet need for FP is 34% [14]. Addressing the unmet need of FP in Ethiopia is expected to avert 12,800 maternal deaths and more than 1.1 million child deaths [15]. The demand for LAFPMs is a critical area of study, particularly in LMICs, like Ethiopia, where the rates of unintended pregnancies remain alarmingly high [16]. Despite providing long-term and efficient family planning options, LAFPMs are frequently underutilized because of a number of obstacles. Improving reproductive health outcomes and lowering mother and newborn morbidity and death linked to unwanted pregnancies require an understanding of the factors that affect demand for these techniques [17,18].
Enhancing access to LAFPMs can significantly decrease the incidence of unsafe abortions and related complications, thereby positively impacting public health [19]. Most of the studies have been conducted on met need of long-acting family planning methods in the general population; however, there was limited number of research on unmet need and demand for long-acting family planning methods among family planning users in Debre Birhane. Similarly, there was no published study conducted to assess the level of demand for long-acting family planning methods and associated factors in Debre Birhane.
Significance of The Study
The evidence-based identification of gaps and related factors for the demand for long-acting family planning and factors among Debre-Birhane family planning users is the main significance of this study. Therefore, based on the degree of influence that the study's findings may have, this study aims to explain the demand for long-acting family planning methods and the factors that influence the target clients' use of such family planning. It also suggests goal-oriented, responsive, and scientific interventions that may increase ownership and commitment among all the relevant bodies to strengthen service utilization.
The findings from this study will help policy makers and planners and other concerned organizations working in the area of family planning and maternal health to meet the demand of long-acting contraceptive methods.
Literature Review
Utilization of Long-Acting Family Planning
By 2020, based on the reproductive health program, the maternal mortality ratio and newborn mortality rate are predicted to decline to 199 maternal deaths per 100,000 live births and 10 deaths per 1,000 live births, respectively, demonstrating the importance of family planning in preventing maternal mortality [20]. Survey in Indonesia show that only slightly over 10% used LAFPMs (implant, IUD) [21]. Study done in Sudan utilization of long-acting family planning are intrauterine devices [10.2%] and Implanon 14% [22]. Utilization family planning Injectable are the most widely used contemporary family planning method among Ethiopian women who are currently married (27%), followed by implants (9%), and the pill and IUD (2
Objectives
General Objectives
- To determine the demand for long-acting family planning methods and identify associated factors among family planning service users in Debre Birhan public health centres, Amhara region, Ethiopia 2025.
Specific Objectives
- To determine the demand for long-acting family planning methods among family planning service users in Debre Birhan public health centers.
- To identify associated factors for the demand of long-acting family planning methods among family planning service users in Debre Birhan public health centers.
Materials and Methods
Study Area and Period
The study was conducted in Debre Birhane public health centers of Amhara region of Ethiopia. Debre Birhane town is located in the northeast part of the Amhara region, and it is 130 km far from Addis Ababa, the capital city of Ethiopia and 695 km away East of Bahir Dar. According to 2022 administrative report, a total population of Debre Birhane is 209, 011.and has five sub city 8 health center 2 public hospital and 1 private hospital and 13 clinics are in Debre Birhane city. The study was conducted from February 1 up to March 30, 2025.in Debre Birhane public health centers.
Study Designs an Institutional Based Cross-Sectional Study Design was Used
Populations
Source Population: All family planning service users reproductive age women of Debre Birhane are the source population from which the study population was drawn.
Study Population: Family planning service users who were selected with a systematic random sampling method from all family planning service users based on a calculated flow rate of service user’s interval was the study population in Debre Birhane governmental health centers.
Study Unit: Family planning service users selected by simple random sampling techniques who was data collected during study period.
Eligibility Criteria
Inclusion Criteria: All women, who are active FP service users, and available in Debre Birhane public health centers during the study period was included.
Exclusion Criteria: Those who are seriously ill and enable to communicate in the study was excluded from the study.
Sample Size Determination
A single population proportion formula is used to determine the total required sample size. The sample is calculated using the assumption of a significance level CI of 95%, a 5% margin of error, and demand for long-acting family planning methods was used from a previous study done in Assosa Town shows that, 62.9% of the respondent had demand for LAFPM. a 62.9% population proportion [42].
A 10% from the total sample is considered or added for a non-response rate. At 95% confidence level (CI), p=0.629, and d= 0.05., N=[(Za/2)2*P (1-P)]/d2, N= [(1.96)2*0.629(1-0.629)]/(0.05)2=358.6 with 10% for non-response rate, then the total sample will be 358.6+ (358.6×10%) = 394.
Table 1: Sample size calculation for the second objective from similar study Utilization of long-acting contraceptive methods and associated factors among married women in Farta Woreda, Northwest Ethiopia.
| Factors | Outcome in un ex | Outcome in ex | CI | Power % | Sample | A % | Total |
| Educational level | 90% | 69.8% | 95% | 80 | 142 | 14 | 156 |
| Previous use of LAFPM | 92.8% | 76.1% | 95% | 80 | 14 | 1 | 15 |
| Attitude | 93.4% | 77.6% | 95% | 80 | 178 | 17 | 195 |
| Having numbers of children | 97.2% | 30.9% | 95% | 80 | 38 | 3 | 41 |
By considering both the first and second objectives the maximum sample size is 358 from the First objective, to get the final sample size with adding the 10% non-respondent rate 358+ (358*10%) =394.the sample size is 394. Since the output for objective one.
Sampling Technique and Procedure
A simple random sampling techniques was used to select the study participants in Debre Berhan public health centers. 5 health centers are randomly selected from 8 health centers in Debre Berhane town. Then, the study participants were selected randomly using a lottery method. The number of study participants was allocated proportionally for each public health centers. Then the respondent subject was selected from selected health centers by using systematic random sampling based on the family planning service client’s flow three months average numbers. The overall sampling procedures and sample allocation techniques looks like in the following table.
Table 2: Sample size proportional allocation for demand for long-acting family planning e methods users in public health centers, Debre Birhane. Ethiopia, 2025.
| Health Centers in Debre Berhane Town Randomly Selects | Average Numbers of Clients for Three Months | Number of Sample Proportional to All |
| 04 Health Center | 1550 | 163 |
| Tebasse HC | 650 | 68 |
| Ayer TenaHC | 715 | 75 |
| Chacha HC | 450 | 47 |
| Minilic HC | 385 | 41 |
| Total | 3750 | 394 |
Debre Birhane city has 8 Health Center Then 5 Health Centre’s selected randomly proportional allocation of Sample drawing selected from health centers.
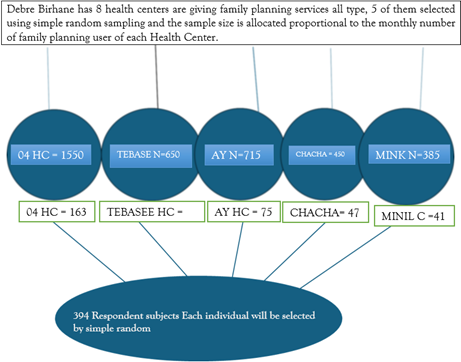
Figure 2: Proportional allocation of Sample drawing techniques for demand for long-acting family planning methods users in public health centers, Debre Birhane. Ethiopia, 2025.
Study Variables
Dependent Variable
Demand of long-acting family planning methods
Independent Variable
- Socio demographic characteristics of clients
- Knowledge of respondent about long-acting family planning method
- Attitude of respondent regarding family planning methods
- Reproductive history of respondent
- Source of information
These independent variables were selected because different previous studies show association with the dependent variable i.e., demand for long-acting family planning.
Operational Definition
LAFPMs: The reversible LAFPMs such as IUD and Implant are considered as LAFPMs.
Demand for LAFPMs: It is determined by adding both the proportion of women who are using long-acting family planning methods (met need) and proportion of women who are using any other short acting family planning methods but want to use LAFPMs (unmet need) [10].
Unmet Need for Long-Acting Family Planning Methods: Women who desired to use Implant or IUCD for spacing or limit pregnancy but did not use the methods due to any reason.
Met Need for Long-Acting Family Planning Methods: Women who use Implant or IUCD.
Attitude: The attitude of women towards LAFPM will be assessed using ten negatively stated attitude related questions, and maximum score was given when participants strongly disagree for the questions and lower points when they strongly agree. The attitude will be labeled as positive attitude for those participants who will be scored above the mean, and negative attitude for those participants who will be scored below or equal to the mean score [14,33)]
Knowledge of Long-Acting Contraceptive Methods: This study suggests that a woman is considered to be good knowledge about long-acting family planning techniques if she cites Mean and above. And poor knowledge is of them answer less than the mean [14].
Data Collection Method
A Structured interview questionnaire was developed from various studies. A clean, and unambiguous questionnaire was prepared in the English language. The questionnaire was translated into the Amharic version. The pretest was conducted 10% of total sample size = 40 at Debre Birhane referral hospital. For each health facility, two data collectors and was recruited and trained. The questionnaire was pre-tested to ensure uniformity. The supervisors and data collectors received adequate training on the data gathering procedure. Supervisors evaluated and verified the completeness of the questionnaires daily throughout the data collecting period, and every other day by the lead investigator and all required input was give. After all the data is collected, the data was entered, labeled, and cleaned using SPSS software.
Data Quality Management
To ensure data quality, all data collectors and supervisors was receiving training and proper orientation before the actual starting of data collection. To maintain consistency, the English version of the questionnaire was translated into the Amharic language and then back into English. Two weeks before the data collection, the questionnaire was pre-tested on 10% of the study population in the Debre Birhane hospital FP unit with a similar population, and a few modifications was made. Furthermore, the accuracy, clarity, and completeness of data was reviewed daily by the principal investigators.
Data Processing and Analysis
The data was undergone verification for completeness, and the Kobo tool box used to data entry and subsequently exported to the SPSS Version 27 software for analysis. Descriptive statistics was calculated, including mean and standard deviation for continuous variables, as well as frequencies and percentages for categorical variables. Check the reliability of the questionnaire and the validity of the variable was tested using Cronbach alpha (0.63 for likert scale variable). Hosmer-lemeshow test is done for goodness of fit and calibration for logistic regression models. Each variable was be assessed for normality and the satisfaction of assumptions utilizing histograms, boxplots, and scatter plots before analysis. The binary logistic regression was used and its assumptions such as multicollinearity and model fitness will be assessed using variance inflation factors (VIF). The results were described using tables, charts, graphs. A variable in bivariate logistic regression with a p-value less than or equal to 0.25 was selected as a candidate for further multivariable analysis. Finally, the association between dependent variables and factors was presented using adjusted odd ratio, and its 95% confidence interval and a p-value of less than 0.05 in multivariable analysis will be consider statistically significant.
Ethical Considerations
Ethical clearance was obtained from the Institutional Review Board (IRB) and supporting latter from Debre Birhane University, Asrat Woldeyes Health Science Campus. A Verbal informed consent was obtained from the study participants. The data privacy and confidentiality were in secured form and used only to meet the objective of this research study. And the study was following the of Debre Birhane university Asrat Woldeyes health compass institutional review board ethical guidelines.
Result Dissemination Plan
The findings disseminated to Debre Birhane University Asrat Woldeyes Health Science Campus department of public health in partial fulfillment for Masters of public health. The findings and recommendations will be distributed to all public health centers, the Debre Birhane town health department and other organizations working on related areas to be used as a baseline for interventions.
Results
Socio-Demographic Characteristics of Respondent
A total of 390 family planning users has participated in this study with response rate of 99%. The mean age of the women was 28.79 and SD ± 5.85 years. Similarly, the majority of 173 (44.4%) of participants were also married. Regarding school enrolment; the majority 168 (43.1%) of the respondents had elementary education, followed by 128 (32.8) with no formal education and the other 69 (17.7%) had some diploma or higher education level. Regarding the occupation status of respondents about 108 (27.7%), were engaged in private business and the rest were government and non-government employees.
Table 3: Socio-demographic characteristics of respondent among women who attend family planning service at public health facilities in Debre Birhane City (2025) (n=390).
| Category | Frequency | Percent % | |
| Age | 15-24 | 145 | 37.2 |
| 25-34 | 152 | 39 | |
| 35-49 | 93 | 23.8 | |
| Marital Status | Single | 81 | 20.7 |
| Married | 173 | 44.4 | |
| Divorced | 24 | 6.6 | |
| Widowed | 112 | 28.7 | |
| Educational Status | No Formal Education | 128 | 32.8 |
| Primary/Elementary | 168 | 43.1 | |
| Secondary | 25 | 6.4 | |
| Diploma and above | 69 | 17.7 | |
| Occupation | Daily Laborer | 33 | 8.5 |
| Government Employee | 86 | 22 | |
| Non-Government Employee | 28 | 7.2 | |
| Housewife | 74 | 19 | |
| Private Business | 108 | 27.7 | |
| Student HighSchool >S | 19 | 4.9 | |
| Unemployed | 42 | 10.8 | |
| Religion | Catholic | 16 | 4.1 |
| Muslim | 63 | 16.2 | |
| Orthodox | 268 | 68.7 | |
| Protestant | 43 | 11 | |
| Husband/Partner Educational Status | No Formal Education | 13 | 3.3 |
| Primary/Elementary | 183 | 46.9 | |
| Secondary | 59 | 15.1 | |
| Diploma and above | 135 | 34.6 |
Demand and Utilization of LAFPM
The current utilization proportion of the demand for LAFPM was 100 (25.6%). Among demanded LAFPM, 35 (35%) met need and 65 (65%) unmet need LAFPM in the town Demand for LAFPM in the study was 100 (25.6%). This was the sum of current use of LAFPM (met need) and the method desired but not used due to any reason (unmet need). Current long-acting family planning users (met need) were 35 (35.0%) and unmet need were 65 (65%).
Table 4: Demand and utilization of LAFPM among women who attend family planning service at public Health facilities in Addis Ababa, 2017(n=390).
| Variables | Options | Frequency | Percen |
| Utilization of LAFPM (Either Implant or IUCD) before | Utilize | 192 | 56.4 |
| Not Utilize | 179 | 43.6 | |
| Demanded LACM (Either IUCD or Implant) current | Demanded | 100 | 25.6 |
| Not Demanded | 290 | 74.4 | |
| Status of Demand Meet | Meet Need | 35 | 35.0 |
| Unmet Need | 65 | 65.0 | |
| Not Demanded | 290 | 74.4 | |
| Ever used implant | Yes | 198 | 50.8 |
| No | 192 | 49.2 | |
| Ever used IUCD | Yes | 22 | 22.6 |
| No | 368 | 77.4 | |
| Ever used any family planning | Yes | 376 | 96.4 |
| No | 14 | 3.6 | |
| Those getinformation about familyplanning method | Yes | 270 | 69.2 |
| No | 120 | 30.8 | |
| Current methodused is by choice | Yes | 274 | 70.25 |
| No | 116 | 29.75 | |
| Waiting Time | Reasonable waiting time | 290 | 74.4 |
| Too long waiting time | 100 | 25.6 |
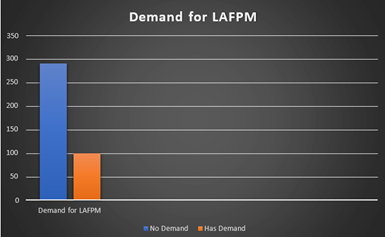
Figure 3: Bar chart show demand to long-acting family planning and has no demand for demand for long- acting family planning methods users in public health centers, Debre Birhane. Ethiopia, 2025.
Reproductive History of The Mother
Regarding the reproductive history of mother; the minimum age at first marriage was 17 years and maximum was 35 years. Similarly, the minimum age at first birth of mothers was 18 years and the maximum was 36 years. Among mothers interviewed, (279, 71.5%) ever gave birth.
Table 5: Reproductive histories of respondent among women who attend family planning service at public health facilities in Debre birhane, 2025 (n=390).
| Category | Frequency | Percent % | |
| Ever gave birth | Yes | 279 | 71.5 |
| No | 111 | 28.5 | |
| Number of births | Nulliparous | 138 | 35.4 |
| Primi (1 birth) | 174 | 44.6 | |
| Multiparty>2 | 78 | 20 | |
| Number of alive children | 0-2 | 64 | 16 |
| 3 or 4 | 38 | 9.7 | |
| >4 | 170 | 43.6 |
Information & Source on Family Planning Methods
Regarding the information on contraceptive method majority (90.3%) of the respondent heard about LAFPM and (49%, 30.7%) mothers have heard about implant and IUCD respectively. Majority (41.4%) of the respondent heard information from health professionals.
Table 6: Health information exposure statues among women who attend family planning service at public health facilities in Debre Birhne (n=390).
| Variable | Category | Frequency | Percent % |
| Ever heardabout long-acting contraceptive method | Yes | 352 | 90.3 |
| No | 38 | 9.7 | |
| Source of information | Health professional | 146 | 41.4 |
| Husband | 78 | 22.2 | |
| Mass media | 73 | 20.7 | |
| Relatives | 55 | 14.1 | |
| If yes what type of LAFPMhave you heard | Implant | 173 | 49 |
| IUCD | 108 | 30.7 | |
| Implant and IUCD | 71 | 20.2 |
Knowledge of Respondents on Family Planning
Regarding the knowledge of women on IUCD method knows that it prevents pregnancy, it does not prevent STI and it does not interfere sexual intercourse (56.9%, 50.5%, 57.7%) respectively. Similarly, knowledge of women on implant knows that it prevents pregnancy, it does not interfere sexual intercourse and pregnancy reverse quickly when implant removed (70%, 58.2% and 30.3%) respectively. Composite score of Knowledge on LAFPM 312 (80%) has good knowledge, and 78 (20%) has Poor knowledge.
Table 7: Knowledge of respondents on family planning methods among women who attend family planning service at public health facilities in Debre birhane (n=390).
| Knowledge Variable | Category | Frequency | Percent % |
| IUCD preventpregnancy | True | 222 | 56.9 |
| False | 67 | 17.2 | |
| Not sure | 101 | 25.9 | |
| IUCD preventSTI | True | 110 | 28.3 |
| False | 197 | 50.5 | |
| Not sure | 83 | 21.3 | |
| IUCD interferes with sexual intercourse or desire | True | 113 | 29 |
| False | 225 | 57.7 | |
| Not sure | 51 | 13.1 | |
| Implant prevent pregnancy | True | 273 | 70 |
| False | 89 | 22.8 | |
| Not sure | 29 | 7.4 | |
| Implant interferes with sexual intercourse or desire | True | 142 | 36.4 |
| False | 227 | 58.2 | |
| Not sure | 21 | 53.8 | |
| Implant reverse pregnancy quickly when removed | True | 118 | 30.3 |
| False | 115 | 29.5 | |
| Not sure | 157 | 40.3 | |
| Composite score of Knowledge on LAFPM | Good knowledge | 312 | 80 |
| Poor knowledge | 78 | 20 |
Attitude of Respondent for LAFPM
In general, about (74.1%, 25.9%) of respondents have positive and negative attitude towards the methods respectively.
Table 8: Attitude of respondents on LAFPM among women who attend family planning service at public health facilities in Debre Birhane health centers (n=390).
| Attitude Variable | Options | Frequency | Percent % |
| Implant causeirregular menses and painful | Agree | 118 | 30.3 |
| Not sure | 147 | 37.7 | |
| Disagree | 125 | 32.1 | |
| IUCD insertion cause loss of privacy | Agree | 64 | 16.4 |
| Not sure | 184 | 47.2 | |
| Disagree | 142 | 36.4 | |
| IUCD restrict normal activity | Agree | 63 | 16.2 |
| Not sure | 135 | 34.6 | |
| Disagree | 192 | 49.2 | |
| Long-acting method safer and more effective than short acting | Agree | 190 | 58.7 |
| Not sure | 141 | 36.2 | |
| Disagree | 59 | 15.1 | |
| Recommend long-acting method to others | Agree | 229 | 58.7 |
| Not sure | 112 | 28.7 | |
| Disagree | 49 | 12.6 | |
| Composite Attitude score of respondents on LAFPM | Positive attitude | 289 | 74.1 |
| Negative attitude | 101 | 25.9 |
Multivariable Analysis
After bivariate analysis variables those shows association at 0.25 level of significance was transferred in to multivariable analysis to control confounding variables and test the association of each variable with the dependent variable. The demand for LAFPM was 100 (25.6%). Among demanded LAFPM, 35 (35%) met need and 65 (65%) unmet need. Age group 35-49 [AOR 2.277(1.452,3.612)], Secondary educational status [AOR 3.638 (1.216,10.886)], No formal education AOR 4.903[1.104,10.777], Unemployed participant [AOR 3.355(2.151,5.126)], Being student 4.885(2.385,6.024), Number of give birth 3 and 4 [AOR 1.795[(0.056,3.73)], Gravida having more than four 0.221(0.061,0.804)], LAFP Methods You heard? [AOR 2.498(1.178, 5.298)] and good attitude [AOR 2.327(1.114, 4.939)] were found predictors of the demand for LAFPM in this study.
Table 9: Multivariable analysis for factors associated with LAFPM among women who attend family planning service at public health facilities in Debre Birhane (n=390).
| Variable | Options | Demand | AOR (95% CI) | |||
| Good Demand % | Poor Demand% | P-value | ||||
| Age | 15-24 | 119 | 26 | 0.01 | 1.00 | 1.00 |
| 25-34 | 113 | 39 | 0.049 | 1.579 (0.199, 2.658) | 1.12 (0.076, 3.543) | |
| 35-49 | 58 | 35 | 0.018* | 2.762 (1.328, 4.997) | 2.277 (1.452, 3.612) | |
| Religion | Catholic | 10 | 6 | 0.020 | 1.00 | 1.00 |
| Muslim | 23 | 10 | 0.666 | 0.725 (0.259, 2.299) | 0.000 | |
| Orthodox | 194 | 54 | 0.929 | 0.464 (0.196, 0.934) | 1.093 (0.192, 6.218) | |
| Protestant | 63 | 20 | 0.59 | 0.529 (0.484, 2.216) | 1.502 (0.290, 7.773) | |
| Education | Elementary | 114 | 14 | 0.001 | 1.00 | 1.00 |
| Secondary | 50 | 19 | 0.003* | 3.094 (2.265, 8.140) | 3.638 (1.216, 10.886) | |
| Diploma and above | 110 | 58 | 0.004 | 4.294 (1.706, 12.295) | 3.278 (0.715, 15.038) | |
| No formal education | 16 | 9 | 0.001** | 4.58 (1.438, 6.658) | 4.903 (1.104, 10.777) | |
| Occupation | Daily laborer | 27 | 6 | 0.434 | 1.00 | 1.00 |
| Government Employee | 43 | 10 | 0.003 | 1.046 (0.486, 5.371) | 1.478 (0.129, 2.924) | |
| Non-government Employee | 36 | 8 | 0.647 | 1.000 (1.753, 3.265) | 2.103 (0.262, 4.889) | |
| House wife | 61 | 13 | 0.047 | 0.959 (0.222, 1.729) | 1.328 (0.268, 3.381) | |
| Private business | 75 | 34 | 0.747* | 2.04 (1.227, 3.894) | 2.450 (1.149, 4.141) | |
| Student high school and above | 34 | 16 | 0.002* | 2.117 (1.015, 6.870) | 4.885 (2.385, 6.024) | |
| Unemployed | 14 | 13 | 0.688* | 4.178 (2.129, 5.868) | 3.355 (2.151, 5.126) | |
| Age at first marriage | 15-24 | 52 | 15 | 0.942 | 1.00 | 1.00 |
| 25-35 | 90 | 57 | 2.195 (1.235, 3.884) | 2.606 (1.221, 4.659) | ||
| How many births have you give? | 0-2 | 160 | 35 | 0.260 | 1.00 | 1.00 |
| 3 and 4 | 111 | 52 | 2.142 (1.309, 3.503) | 8.976 (2.596, 13.671) | ||
| >4 | 19 | 13 | 3.128 (1.413, 6.924) | 4.286 (2.776, 9.685) | ||
| How many of them are alive? | 0-2 | 149 | 28 | 1.00 | 1.00 | |
| 3 and 4 | 118 | 57 | 0.050 | 2.571 (1.539, 4.293) | 1.795 (0.056, 3.73) | |
| >4 | 23 | 15 | 0.260* | 3.470 (1.614, 7.462) | 0.221 (0.061, 0.804) | |
| Have you ever had exposure to long-acting contraceptive message through mass media within the last 12 months? | Yes | 128 | 18 | 0.001 | 1.00 | 1.00 |
| No | 162 | 82 | 3.599 (1.159, 5.487) | 3.244 (1.294, 4.23) | ||
| If yes, please mention LAFP Methods You heard? | Implanon | 144 | 26 | 1.00 | 1.00 | |
| IUCD | 116 | 66 | 3.151 (1.882, 5.277) | 2.498 (1.178, 5.298) | ||
| Attitude | Poor attitude | 85 | 16 | 1.00 | 1.00 | |
| Good attitude | 205 | 84 | 0.010* | 2.177 (1.254, 4.830) | 2.327 (1.114, 4.939) | |
Discussion
The study assessed the demand for long-acting family planning methods and associated factors among family planning service users in public health centers, Debre Birhan. Regarding the age, marital and educational statuses of the respondent majority were age between (25-34) (152)39%, Marriage (173)44.1%, and has primary level educational status (168)43.1%. In general, about (74.1%, 25.9%) of respondents have positive and negative attitude towards the methods respectively. According to this research finding in Debre birhane Selected health center family planning unit this study shows that, Demand for long-acting family planning 100(25.6%). Among demanded LAFPM, 35(35%) met need from the demand but it is 9% meet need from the total respondents and 65 (65%) unmet need from demand total or the un meet need is 16.6% out of total participant, of women were using short acting methods while they actually want to use long-acting methods (unmet need). And the rest are no demand to use LAFPM at all. Regarding the reproductive history of mother; the minimum age at first marriage was 17 years and maximum was 35 years. Similarly, the minimum age at first birth of mothers was 18 years and the maximum was 36 years. Among mothers interviewed, (279, 71.5%) ever gave birth. Regarding the information on contraceptive method majority (90.3%) of the respondent heard about LAFPM and (49%, 30.7%) mothers have heard about implant and IUCD respectively. Majority (41.4%) of the respondent heard information from health professionals. Regarding the knowledge of women on IUCD method knows that it prevents pregnancy, it does not prevent STI and it does not interfere sexual intercourse (56.9%, 50.5%, 57.7%) respectively. Similarly, knowledge of women on implant knows that it prevents pregnancy, it does not interfere sexual intercourse and pregnancy reverse quickly when implant removed (70%, 58.2% and 30.3%) respectively. Composite score of Knowledge on LAFPM 312(80%) has good knowledge, and 78(20%) has Poor knowledge.
This result show that lower than A survey study from Iran show that the demand of Modern family planning methods is 71.35%, and only 27.7% of women use LAFPMs [26], and it is higher result when compare with Study in south Africa show that women have limited autonomy to choose or to use contraception or the method that they might prefer [27]. This difference may due to the Ethiopian women has right to use any of the select family planning method.
This study has higher demand of Long-acting family planning demand when compare with A study in Kenya shows that only 18% of women utilize LAFPMs [28]. In this study 352(90.3%) respondent heard about FP service and better when compare with A study done in Uganda show that 4% of mothers never heard about the FP services [29]. Another study in Nigeria shows that 38.7% of women utilize LAFPMs [30]. The difference is may be because of in south Africa show that women have limited autonomy to choose or to use contraception, population difference and time gap. This study is higher result long-acting family planning methods when compare with A study from Nepal show that 11% reproductive age women uptake LACMs [32]. There for this study is better result than study done Studies from Northwest Ethiopia show that the demand of LAFPMs is 17% [10], and 14.3% [33].
This study result is near to similar A study from Oromia region of Ethiopia show that 28.4% of reproductive women utilize LAFMS [34]. And Various studies in the Amhara region of Ethiopia show that this study lower result that of 51.1% of reproductive-age women receive LACMs in West Gojam shows [7], 16.3% in Bonbe District [35], 34.7% in Gondar City [37], 17.6% in Dendi District [37], and 12.9% in Janamora District [38]. May the difference make different factors population variation and time of study.
Study done in Debre Tabore show that the less thane this study result demand for long-acting contraceptive methods was 17%. This was the sum of current use of long-acting contraceptive methods (met need) and the method desired but not used due to any reason (unmet need). Current long-acting family planning users (met need) were 9.2% and unmet need were 7.8%, out of the total short acting contraceptive method users, 7.8% of the participants did not prefer to use short acting family planning methods [39]. Enhancing those elements is used to raise demand. Women who are in demand are those who are between the ages of 35 and 49, have several gravidas, and so providing information about long- acting family planning through the media can either increase the number of women utilizing long-acting techniques or boost demand. This study indicates a lower demand for LAFPM compared to a previous study in Assosa Town, which found that 62.9% of respondents expressed a need for it. Overall, there is a low demand for LAFPM and a significant unmet need.
The following factors were positively correlated with the demand for LAFPMs: marital status, multigravida, media information, attitude toward LAFPM, age 35-49, and education. No formal schooling, 25-35 years old when married, and a student. Impact the study's requirement for LAFPM. Debre Birhane research findings According to this study's selected health center family planning unit, the demand for long-acting family planning 100(25.6%) is less than According to a study conducted in the Sidama region, 37.8% of study participants (95% CI: 32.9-42.7) used reversible long-acting family planning. Of them, 36(9.6%) used IUCD and 106(28.0%) used implants [23]. It is May due to population and time difference. The result of this study is also lower than study done in Study done in Addis Ababa demand for LAFPM a study was high and the unmet need for LAFPM also high. Marital status, gravidity, information on LAFPM, knowledge on LAFPM, attitude on LAFPM is affect the demand for LAFPM
in this study. The demand for LAFPM was 650(76.7%). Among demanded LAFPM, 305(36%) meet need and 345(40.7%) unmet need [24]. Also, the variation may be due to different study, population and time difference. Age group 35-49 AOR 2.277(1.452,3.612), Those who have Secondary educational status [AOR 3.638[1.216,10.886], No formal education AOR 4.903[1.104,10.777], un Employed participant AOR 3.355[2.151,5.126], Being student at high school and above and reproductive age group 4.885[2.385,6.024], Number of give birth 3 and 4 [AOR 1.795[(0.056,3.73)], Gravida having more than four 2.22[0.061,0.804], heard about LAFP Methods [AOR 2.498[1.178, 5.298] and Good attitude [AOR 2.327[1.114, 4.939] were found predictors of the demand for LAFPM in this study. According to knowledge 312(80%) of respondent has good knowledge about long-acting family planning.
This result is higher than study done in Debre Tabor survey. Study done in Debre Tabore show that the less thane this study result demand for long-acting contraceptive methods was 17%. Just 9.2% of women were using long-acting contraceptive methods (meet need). 7.8% of women were adopting short acting skills, despite their wish (unmet) to use extended acting strategies. In this study those who are Secondary educational status has 3.64 times more has demand to use long-acting family planning this result is higher indicator when compare with a study report from Gondar City shows that women with above secondary education are 2.91 times more likely to utilize LAFPMs than their counterparts [36]. Differently to other studies at this study show that being student at high school and above and reproductive age group 4.8 time has demand to long-acting family planning method when compare with women has other occupation.
Study done in oromia the women under 20 years of age are 1.78 times more likely to use LAFPMs compared to women age above 20 years [43]. Unlikely on this study how that Age group 35-49 AOR
2.28 time has demand to use long-acting family planning method.
Study done in gonder women who have information about LAFPM are 8.85 times more likely to utilize LAFPMs than their counterparts [36]. Heard about LAFP Methods 2.5-time times more likely to utilize LAFPMs this result show that there is information and knowledge gap difference between two study areas. Multi Gravida having more than four pregnancies has 2.22 times demand to use long-acting family planning when compare with those has only one pregnancy. Lower when compare with study done in Mekelle study Compared to mothers who had only been pregnant once, those who had two or more pregnancies were three times more likely to utilize LAFP (AOR = 2.7, 95%: 1.4, 5.1). Another study included factors such as age, length of time desired to have children, number of children born knowledge about and use of modern FP, and spousal conversations during the previous six months [14]. The demand for LAFPM similarly with this study was positively correlated with having five or more children or multi gravida women (AOR = 1.67, 95% CI = [1.58, 4.83]), choosing to use the methods with husbands (AOR = 2.73, 95% CI = [1.40, 5.32]), being a student high school and above (AOR = 2.64, 95% CI = [1.27, 5.47]), not planning to have children in the future (AOR = 2.17, 95% CI = [1.12, 4.23]), being a daily worker (AOR = 3.87, 95% CI = [1.06, 14.20]), and frequently speaking with husbands. Patients not being treated well by medical personnel [10]. According to this study, people with a good attitude are 2.33 times more likely to have demand than people with a bad attitude. This finding is almost identical to a study conducted in Farta Woreda, Northwest Ethiopia: Women with an optimistic outlook and those with low wealth are 2.74 and 3.39 times more likely to seek the use of LAFPMs, respectively [33]. Study done in Asosa heard about LAFPM Methods higher significant 3.37 time has demand to LAFPM In this study heard about LAFP Methods [AOR 2.498[1.178, 5.298] [42]. The possible reason for the variation of the result might be due to different geographical location, increased globalization and may also due to different study period.
Strength and Limitation of Study
Strength of Study
- The questioner was pretested on similar setting and possessed high response rate and employed a straightforward random sample technique, the sampling strategy and process reduced selection bias.
Limitation of The Study
- The limitation of this study was cross-sectional nature of the data that temporal relationship between exposure and outcome variable could not be established
- This study was conducted among only family planning service users in the government facilities; it may not representative to general population.
Conclusion
Demand of LAFPM was found low 100 (25.6%) among women in Debre Birhane who attended family planning service in public health facilities. Factor which are associated with long-acting family planning method are Gravida status, Multigravida, Information from mass media, attitude on LAFPM, Age 35-49 education No formal education age at marriage 25-35 and being student. And No employment show association with demand for LACM by the bivariate analysis.
Recommendation to Debre Birhane Health Department
- Having positive attitude for LAFPM show high demand for LAFPM compared to those who have negative attitude so it is better to address the attitude of community on birth control effect of LAFPM, as it has less side effect compared to others, and give information clearly to the community by using Information from mass media, Health centers.
- Expected to do more to Arrange time and place where short and brief health education related to family planning especially LAFPM can be given for those clients who come to the institution for family planning, ANC, safe abortion care service and postnatal mother come for vaccine.
- Assign and continuously follow those health care providers who were assigned to provide health education related to reproductive health mainly long-acting family planning to those who have 3 and more birth, No formal education, and age at marriage 25-35.
- To do more by assigning health care provider to provide the outreach health education program related to the role of Long-acting family planning and counselling’s session to the community reproductive women’s, husband and any concerned body who play role in the contraceptive utilization.
Community Leaders
Expected to do more to increase the involvement of husband or partners on shared decision making and give them education related to the role of family planning to maintain reproductive health at different setting like social meeting area in the community (Idir, conference and the like).
Research Institutes and Researchers
A more intense qualitative and quantitative studies especially in the community settings are needed to gain further insight on acceptance of Long-term family planning by reproductive women, their husband and community religious leaders.
References
- WHO. (2025). Family Planning/Contraception Methods. World health Organization.
Publisher | Google Scholor - Cates Jr, W., Stanback, J., Maggwa, B. (2014). Global Family Planning Metrics-Time for New Definitions? Contraception, 90(5):472-475.
Publisher | Google Scholor - Cleland, J., Bernstein, S., Ezeh, A., Faundes, A., Glasier, A., et al. (2006). Family Planning: The Unfinished Agenda. The Lancet, 368(9549):1810-1827.
Publisher | Google Scholor - Phethi, C. (2021). A Qualitative Exploration on Use of Long-Acting Reversible Contraceptives Among Married Women at MZIMBA South District Hospital (Master's Thesis, Kamuzu University of Health Sciences (Malawi)).
Publisher | Google Scholor - Starbird, E., Norton, M., Marcus, R. (2016). Investing in Family Planning: Key to Achieving the Sustainable Development Goals. Global Health: Science and Practice, 4(2):191-210.
Publisher | Google Scholor - Islam, M. R. (2024). Family Planning and Sustainable Development Goals. In Family Planning and Sustainable Development in Bangladesh: Empowering Marginalized Communities in Asian Contexts. Emerald Publishing Limited. 155-175.
Publisher | Google Scholor - Zeleke, E. D., Assefa, D. G., Woldesenbet, T. T., Gido, R., Mengistu, N., et al. (2022). Utilization of Long Acting and Permanent Contraceptive Methods and Associated Factor Among Women of Reproductive Age in West Guji Zone, Southwest Ethiopia. Reproductive Health, 19(1):31.
Publisher | Google Scholor - Coulson, J., Sharma, V., Wen, H. (2023). Understanding the Global Dynamics of Continuing Unmet Need for Family Planning and Unintended Pregnancy. China Population and Development Studies, 7(1):1-14.
Publisher | Google Scholor - Wulifan, J. K., Brenner, S., Jahn, A., De Allegri, M. (2015). A Scoping Review on Determinants of Unmet Need for Family Planning Among Women of Reproductive Age in Low- and Middle-Income Countries. BMC Women's Health, 16(1):2.
Publisher | Google Scholor - Yalew, S. A., Zeleke, B. M., Teferra, A. S. (2015). Demand for Long-Acting Contraceptive Methods and Associated Factors Among Family Planning Service Users, Northwest Ethiopia: A Health Facility Based Cross Sectional Study. BMC Research Notes, 8(1):29.
Publisher | Google Scholor - Fekadu, G. A., Omigbodun, A. O., Roberts, O. A., Yalew, A. W. (2019). Factors Associated with Long Acting and Permanent Contraceptive Methods Use in Ethiopia. Contraception and Reproductive Medicine, 4(1):9.
Publisher | Google Scholor - Arimond, M., Ruel, M. T. (2002). Progress in Developing an Infant and A Child Feeding Index: An Example Using the Ethiopia Demographic and Health Survey 2000.
Publisher | Google Scholor - Ethiopia Fmoh. (2017). From MDGs to SDGs: Remaining Challenges to Implementation of Reproductive Health Programmes in Ethiopia.
Publisher | Google Scholor - Alemayehu, M., Belachew, T., Tilahun, T. (2012). Factors Associated with Utilization of Long Acting and Permanent Contraceptive Methods Among Married Women of Reproductive Age in Mekelle Town, Tigray Region, North Ethiopia. BMC Pregnancy and Childbirth, 12(1):6.
Publisher | Google Scholor - Initiative UHP. (2009). The Contribution of Family Planning, Achieving MDGs in Ethiopia.
Publisher | Google Scholor - Abubakar, H. Y. (2023). Determinants Impacting the Adoption of Long-Acting Contraception among Women in Fort Portal Regional Referral Hospital's MCH Clinic, IAA Journal of Applied Sciences. 10(1):122-129.
Publisher | Google Scholor - Malarcher, S., Olson, L. G., Hearst, N. (2010). Unintended Pregnancy and Pregnancy Outcome: Equity and Social Determinants. Equity, Social Determinants and Public Health Programmes, 2:177-197.
Publisher | Google Scholor - Khan, M. N., Harris, M. L., Shifti, D. M., Laar, A. S., Loxton, D. (2019). Effects of Unintended Pregnancy on Maternal Healthcare Services Utilization in Low-and Lower-Middle-Income Countries: Systematic Review and Meta-Analysis. International Journal of Public Health, 64(5):743-754.
Publisher | Google Scholor - Mohamed SF. (2024). Enhancing Utilization of Long-Acting Contraceptive Methods among Women: A Study in Hoima Regional Referral Hospital, IDOSR Journal of Biology, Chemistry and Pharmacy, 9(1):11-20.
Publisher | Google Scholor - Titaley, C. R., Sallatalohy, N. (2020). Utilization of Family Planning Contraceptives Among Women in The Coastal Area of South Buru District, Maluku, 2017. Kesmas: Jurnal Kesehatan Masyarakat Nasional (National Public Health Journal), 15(1):40-47.
Publisher | Google Scholor - Ibnouf, A. H., Van den Borne, H. W., Maarse, J. A. M. (2007). Utilization of Family Planning Services by Married Sudanese Women of Reproductive Age. EMHJ-Eastern Mediterranean Health Journal, 13(6):1372-1381.
Publisher | Google Scholor - Gujo, A. B., Kare, A. P. (2021). Utilization of Long-Acting Reversible Contraceptives and Associated Factors Among Reproductive Age Women Attending Governmental Health Institutions for Family Planning Services in Wondo Genet District, Sidama, National Regional State, Southern Ethiopia. Health Services Research and Managerial Epidemiology, 8:23333928211002401.
Publisher | Google Scholor - Debella.pdf B. (2017). Demand for Long-Acting Family Planing and Associated Factors Selected Public Health Centers Addis Ababa Ethiopia.
Publisher | Google Scholor - Wondie, K. Y., Badi, M. B., Tamiru, A. T. (2020). Rural-Urban Differentials of Long-Acting Contraceptive Method Utilization Among Reproductive-Age Women in Amhara Region, Ethiopia: Further Analysis of The 2016 EDHS. Open Access Journal of Contraception, 77-89.
Publisher | Google Scholor - Hosseini, H., Torabi, F., Bagi, B. (2014). Demand for Long-Acting and Permanent Contraceptive Methods Among Kurdish Women in Mahabad, Iran. Journal of Biosocial Science, 46(6):772-785.
Publisher | Google Scholor - Kriel, Y., Milford, C., Cordero, J. P., Suleman, F., Steyn, P. S., et al. (2021). Quality of Care in Public Sector Family Planning Services in KwaZulu-Natal, South Africa: A Qualitative Evaluation from Community and Health Care Provider Perspectives. BMC Health Services Research, 21(1):1246.
Publisher | Google Scholor - Kungu, W., Khasakhala, A., Agwanda, A. (2020). Use of Long-Acting Reversible Contraception Among Adolescents and Young Women in Kenya. PLoS One, 15(11):e0241506.
Publisher | Google Scholor - Idere, G. P. (2019). Factors Affecting Utilization of Family Planning Services Among Mothers Delivering at Fort Portal Regional Referral Hospital, Uganda.
Publisher | Google Scholor - Mohammed-Durosinlorun, A., Adze, J., Bature, S., Abubakar, A., Mohammed, C., et al. (2017). Uptake and Predictors of Long-Acting Reversible Contraceptives Among Women in A Tertiary Health Facility in Northern Nigeria. Journal of Basic and Clinical Reproductive Sciences, 6(2).
Publisher | Google Scholor - CSA-Ethiopia. (2012). Ethiopia Demographic and Health Survey 2011. Central Statistical Agency of Ethiopia and ICF International Addis Ababa, Ethiopia and Calverton, Maryland, USA.
Publisher | Google Scholor - Mehata, S., Bhattarai, N., Menzel, J., Shah, M., Khanal, P., et al. (2019). Prevalence and Correlates of Postabortion Long-Acting Reversible Contraceptive (LARC) Use Among Young Women (24 and below) in Nepal: Strategy in The Search for Improvements. Reproductive Health, 16(1):55.
Publisher | Google Scholor - Aychew, E. W., Bekele, Y. A., Ayele, A. D., Dessie, A. M., Dagnew, G. W. (2022). Utilization of Long-Acting Contraceptive Methods and Associated Factors Among Married Women in Farta Woreda, Northwest Ethiopia: A Community-Based Mixed Method Study. BMC Women's Health, 22(1):533.
Publisher | Google Scholor - Mota, K., Reddy, S., Getachew, B. (2015). Unmet Need of Long-Acting and Permanent Family Planning Methods Among Women in The Reproductive Age Group in Shashemene Town, Oromia Region, Ethiopia: A Cross Sectional Study. BMC Women's Health, 15(1):51.
Publisher | Google Scholor - Geta, W., Asseffa, N. A., Mekonnen, N. (2018). Utilization of Long Acting and Permanent Contraceptive Methods and Associated Factors Among Married Childbearing Age Women in Bombe District, Southern Ethiopia. Reprod Syst Sex Disord, 7(01):1-9.
Publisher | Google Scholor - Zenebe, C. B., Adefris, M., Yenit, M. K., Gelaw, Y. A. (2017). Factors Associated with Utilization of Long-Acting and Permanent Contraceptive Methods Among Women Who Have Decided Not to Have More Children in Gondar City. BMC Women's Health, 17(1):75.
Publisher | Google Scholor - Sahilemichael, A., Temesgen, K. Gemechukejela. (2015). Determinants of Long-Acting Reversible Contraceptives Use among Child Bearing Age Women in Dendi District, Western Ethiopia. J Women’s Health Care, 4(242):2167-0420.
Publisher | Google Scholor - Assemie, M. A., Muchie, K. F., Ayele, T. A. (2018). Incidence and Predictors of Loss to Follow Up Among HIV-Infected Adults at Pawi General Hospital, Northwest Ethiopia: Competing Risk Regression Model. BMC Research Notes, 11(1):287.
Publisher | Google Scholor - Yalew, S. A., Zeleke, B. M., Teferra, A. S. (2015). Demand for Long-Acting Contraceptive Methods and Associated Factors Among Family Planning Service Users, Northwest Ethiopia: A Health Facility Based Cross Sectional Study. BMC Research Notes, 8(1):29.
Publisher | Google Scholor - Takele, A., Degu, G., Yitayal, M. (2012). Demand for Long Acting and Permanent Methods of Contraceptives and Factors for Non-Use Among Married Women of Goba Town, Bale Zone, South East Ethiopia. Reproductive Health, 9(1):26.
Publisher | Google Scholor - Bolarinwa, O. A., Afaya, A., Ajayi, K. V., Ojo, A., Alawode, O. A. (2022). Prevalence and Factors Associated with The Use of Long-Acting Reversible and Permanent Contraceptive Methods Among Women Who Desire No More Children in High Fertility Countries in Sub-Saharan Africa. BMC Public Health, 22(1):2141.
Publisher | Google Scholor - Birku, Z., Berhe, S., Assefa, Y. (2021). Demand for Long Acting and Permanent Contraceptives Methods and Associated Factors Among Married Women Visiting Assosa Town Health Institution for Family Planning. Journal of Family Medicine and Health Care, 7(3):65-76.
Publisher | Google Scholor - Mekonnen, F. A., Mekonnen, W. N., Beshah, S. H. (2017). Predictors of Long Acting and Permanent Contraceptive Methods Utilization Among Women in Rural North Shoa, Ethiopia. Contraception and Reproductive Medicine, 2(1):22.
Publisher | Google Scholor - Gizaw, A., Regassa, N. (2011). Family Planning Service Utilization in Mojo Town, Ethiopia: A Population-Based Study. Journal of Geography and Regional Planning, 4(6):355.
Publisher | Google Scholor - Aychew, E. W., Bekele, Y. A., Ayele, A. D., Dessie, A. M., Dagnew, G. W. (2022). Utilization of Long-Acting Contraceptive Methods and Associated Factors Among Married Women in Farta Woreda, Northwest Ethiopia: A Community-Based Mixed Method Study. BMC Women's Health, 22(1):533.
Publisher | Google Scholor























