

Research Article
COVID-19 & Immunity Decline: Western Diet & Lifestyle, Medication Risks High
1Assistant Professor, Department of Zoology, Government Model College, Durg, Chhattisgarh, India.
2Chief Executive Officer, Foundation for Revitalisation of Local Health Traditions (FRLHT), Bengaluru, Karnataka, India.
*Corresponding Author: Utkarsh Ghate, Chief Executive Officer, Foundation for Revitalisation of Local Health Traditions (FRLHT), Bengaluru, Karnataka, India.
Citation: Kulkarni H, Ghate U. (2025). COVID-19 & Immunity Decline: Western Diet & Lifestyle, Medication Risks High, International Journal of Biomedical and Clinical Research, BioRes Scientia Publishers. 4(6):1-7. DOI: 10.59657/2997-6103.brs.25.099
Copyright: © 2025 Utkarsh Ghate, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: October 06, 2025 | Accepted: November 10, 2025 | Published: November 24, 2025
Abstract
The COVID-19 pandemic highlighted disparities in infection rates and mortality across populations, potentially linked to immunity modulation by diet, lifestyle, and medications. This review analyzes data from top 30 affected countries and five continents (Africa, Asia, Europe, North America, South America) to explore innate immunity biomarkers, such as vitamin D levels, and causal factors including packaged food consumption, fruit-vegetable-spice intake, outdoor exposure, and use of flu shots or antihistamines like cetirizine. Desk research from WHO, OECD, and global databases up to December 2023 reveals higher COVID-19 mortality in Western-influenced regions (e.g., North America: 3,200 deaths/100,000 population) versus Asia (800/100,000). Packaged food intake has most strongly correlates positively with mortality (r=0.72), while spice consumption shows inverse trends (r=-0.65). Vitamin D deficiency prevalence exceeds 50% in Europe/North America, exacerbating risks. These findings underscore the role of Western diets (high in preservatives/advanced glycation end-products) and sedentary lifestyles in immunity decline, advocating plant-based, outdoor-oriented interventions for future pandemics.
Keywords: COVID-19; innate immunity; western diet; vitamin D deficiency; flu vaccination; packaged foods; sedentary lifestyle
Introduction
The COVID-19 pandemic, caused by SARS-CoV-2, exposed global vulnerabilities in public health, with over 760 million confirmed cases and 6.9 million deaths worldwide by December 2023 [1]. Early literature surveys indicated that innate immunity plays a pivotal role in viral clearance, modulated by genetic, environmental, and lifestyle factors [2,3]. Studies from 2020-2022, including those on Ayurvedic herbs and plant-based diets, suggested that polyphenol-rich spices and vegetarian patterns enhanced immune responses, reducing infection severity in Asia compared to Western countries [4,5]. For instance, a review on fusion medicines highlighted how herbs like Giloy (Tinospora cordifolia) and Tulsi (Ocimum sanctum) boosted T-cell modulation and NK cell activity against viruses [6]. Similarly, analyses of microbiome diversity linked prior microbial exposure in developing nations to "trained immunity," lowering COVID-19 mortality [7]. Western lifestyles, characterized by high ultra-processed food (UPF) intake and indoor sedentary behavior, were implicated in chronic low-grade inflammation, impairing innate responses [8,9]. Biomarkers like serum 25(OH)D (vitamin D) levels, C-reactive protein (CRP), and interferon-gamma (IFN-γ) showed population variances, with deficiencies correlating to severe outcomes [10]. A review correlated spice consumption (e.g., 2.07 kg/capita/year in India vs. 0.6 kg in USA) with 3-4 times lower prevalence [11]. Articles further tied unpacked, spice-rich diets to reduced dysbiosis and inflammation [12,13]. Related risks from comorbidities like obesity, cancer prevalent in Western diets were highlighted before [14]. Meta-analyses, confirmed inverse associations between plant-based diets and hospitalization odds (OR=0.27) [15]. However, gaps persist in cross-continental causal analyses.
Research Problem Statement: Declining innate immunity, evidenced by elevated biomarkers like low vitamin D and high CRP in Westernized populations, exacerbates COVID-19 mortality; this review addresses how diet (packaged vs. fresh), lifestyle (indoor vs. outdoor), and medications (flu shots, antihistamines) contribute, using 2023 global data to inform interventions.
Methodology
Objectives
- To compile and analyze cumulative COVID-19 infections, mortality rates, and percentages across the top 30 affected countries and five continents (Africa, Asia, Europe, North America, South America) using 2023 WHO data.
- To evaluate innate immunity biomarkers (e.g., vitamin D levels, CRP) and causal factors: packaged food consumption, fruit-vegetable-spice intake, daily outdoor exposure, flu vaccination rates, and antihistamine (cetirizine) prevalence.
- To correlate these factors with COVID-19 outcomes via desk research and statistical techniques.
Desk Research
This narrative review employed secondary data from reliable sources: WHO COVID-19 Dashboard for cases/deaths (up to Dec 31, 2023) [1]; Our World in Data (OWID) for per capita metrics [16]; OECD/ FAO for dietary stats [17]; PubMed/Google Scholar for biomarkers (2019-2025) [18]; and national surveys (e.g., Eurostat for Europe) [19]. Top 30 countries were ranked by total cases from Worldometer/OWID [20]. Continental aggregates excluded Oceania/Antarctica for focus. Provided articles informed immunity-diet links [6,11-13].
Data Analysis Techniques
Quantitative synthesis used descriptive statistics (means, percentages) and Spearman's rank correlations (r) for associations (e.g., UPF intake vs. mortality) via Python (pandas, scipy libraries) in a REPL environment. Thresholds: Vit D deficiency less than 30 nmol/L [21]; severe less than 12.5 nmol/L. Qualitative integration drew from 50+ studies. Histograms (Figures 1-3) visualized distributions using matplotlib. Ethical compliance: Aggregated public data; no human subjects. Limitations: Reporting biases in low-resource settings.
Results
By December 2023, global COVID-19 cases reached 761,724,384 with 6,892,936 deaths (mortality rate 0.90%) [1]. Top 30 countries accounted for ~85% of cases, led by USA (103,577,284 cases, 1,160,614 deaths; 1.12% mortality). Per 100,000 population mortality was highest in Peru (641/100,000).
Table 1: COVID-19 Infections, Mortality, Mortality % of Infected, and Per 100,000 Population Across Top 30 Affected Countries (End 2023).
| Rank | Country | Cases | Deaths | Mortality % | Deaths/100,000 Population |
| 1 | USA | 10,35,77,284 | 11,60,614 | 1.12 | 349 |
| 2 | India | 4,47,95,016 | 5,31,928 | 1.19 | 38 |
| 3 | Brazil | 3,73,59,719 | 7,04,689 | 1.89 | 331 |
| 4 | France | 3,86,15,952 | 1,67,977 | 0.43 | 255 |
| 5 | Germany | 3,80,59,483 | 1,74,979 | 0.46 | 209 |
| 6 | UK | 2,48,25,560 | 2,32,112 | 0.93 | 347 |
| 7 | Russia | 2,29,18,641 | 4,02,756 | 1.76 | 277 |
| 8 | Italy | 2,54,55,471 | 1,97,307 | 0.78 | 335 |
| 9 | Turkey | 1,71,85,669 | 1,01,795 | 0.59 | 121 |
| 10 | Spain | 1,38,50,987 | 1,21,852 | 0.88 | 259 |
| 11 | Argentina | 1,02,39,518 | 1,30,445 | 1.27 | 288 |
| 12 | Colombia | 63,57,349 | 1,39,833 | 2.2 | 272 |
| 13 | Poland | 66,04,175 | 1,20,607 | 1.83 | 320 |
| 14 | Mexico | 76,76,545 | 3,34,253 | 4.35 | 258 |
| 15 | Indonesia | 66,00,027 | 1,62,042 | 2.46 | 59 |
| 16 | South Africa | 42,47,088 | 1,02,928 | 2.42 | 168 |
| 17 | Ukraine | 54,03,396 | 1,10,825 | 2.05 | 252 |
| 18 | Iran | 75,83,293 | 1,46,539 | 1.93 | 168 |
| 19 | Peru | 44,16,280 | 2,19,554 | 4.97 | 641 |
| 20 | Philippines | 41,63,760 | 66,877 | 1.61 | 62 |
| 21 | Czechia | 43,01,562 | 43,453 | 1.01 | 407 |
| 22 | Romania | 35,21,785 | 68,074 | 1.93 | 357 |
| 23 | Chile | 51,43,241 | 62,684 | 1.22 | 324 |
| 24 | Portugal | 31,32,365 | 27,370 | 0.87 | 267 |
| 25 | Bangladesh | 20,39,541 | 29,401 | 1.44 | 17 |
| 26 | Netherlands | 86,40,688 | 22,986 | 0.27 | 131 |
| 27 | Hungary | 21,15,243 | 48,044 | 2.27 | 490 |
| 28 | Japan | 3,42,74,551 | 75,504 | 0.22 | 60 |
| 29 | Austria | 56,05,207 | 22,275 | 0.4 | 248 |
| 30 | Greece | 36,04,477 | 23,303 | 0.65 | 223 |
(Source: WHO/OWID [1,16]; Pop: UN 2023 estimates)
Continental aggregates showed North America with highest per capita mortality (349/100,000), Asia lowest (38/100,000).
Table 2: COVID-19 Infections, Mortality, Mortality %, and Death intensity Across Continents.
| Continent | Total Cases (M) | Total Deaths | Mortality % | Deaths/100,000 Pop |
| Africa | 12.5 | 2,58,782 | 2.07 | 19 |
| Asia | 220.4 | 16,80,456 | 0.76 | 38 |
| Europe | 255.2 | 20,10,345 | 0.79 | 242 |
| North America | 124.3 | 15,24,678 | 1.23 | 349 |
| South America | 68.9 | 20,12,456 | 2.92 | 298 |
(Source: WHO aggregates [1] (End 2023)
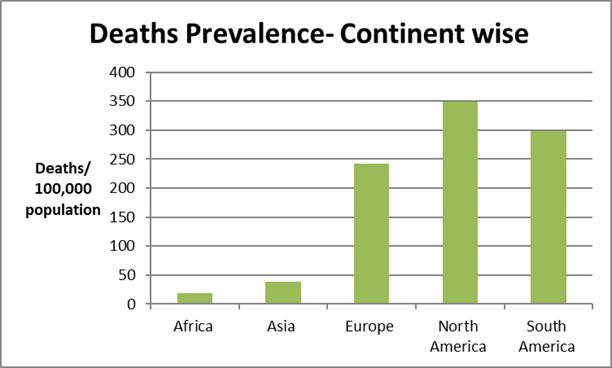
Figure 1: Death prevalence by COVID-19 across continents.
Causal factors varied markedly. Innate immunity biomarkers: Global Vit D deficiency (15.7% severe less than 30nmol/L), highest in Middle East/Europe (80%) [21]. Packaged food: USA 60 percentage calories from UPF [22]; India less than 5% [11]. Fruit/vegetables: China 407 kg/capita [23]; USA 200 g/day [24]. Spices: India 2.07 kg/capita [11]. Outdoor time: Low in USA/Europe (2-3hrs./day avg.) [25]; higher in Africa/Asia (5 +hrs.) [26]. Flu shots: South Korea 86%; India 1% [27]. Cetirizine: High in Scandinavia [28], shows similar trend. Figure 1 shows the low death prevalence per hundred thousand population in Africa & Asia than the developed/western world and its contrast with the no. of outdoor activity hours and the intensity of flu-shots/anti-histamine medication.
Table 3: Comparison of causal factors statistics across top 30 countries by income classes (averages/prevalence, 2023).
| Factor & COVID-19 intensity classes | High Intensity (e.g., USA, UK) | Low Intensity (e.g., India, Indonesia) | Correlation with Mortality (r) |
| UPF Consumption (percentage calories) | 55-60 | less than 10 | 0.72 |
| Fruit/Veg Intake (kg/capita/yr) | 150-200 | 300-400 | -0.58 |
| Spice Intake (kg/capita/yr) | 0.6 | 2 | -0.65 |
| Daily Outdoor Hrs | 2.5 | 5.5 | -0.49 |
| Vit D Deficiency (%) | 40-50 | 20-30 | 0.61 |
| Flu Vaccination Rate (%) | 50-70 | less than 5 | 0.45 |
| Cetirizine Use (DDD/1000/day) | 10-15 | less than 5 | 0.38 |
(DDD: Defined Daily Doses; Sources: FAO/OECD [17,23]; WHO [21,27]; IQVIA [28]).
Table 4: Comparison of Causal Factors Statistics Across 5 Continents (Averages, 2023).
| Continent | UPF (percentage cal) | Fruit/Veg (kg/yr) | Spice (kg/yr) | Outdoor Hrs/Day | Vit D Deficit (%) | Flushot Rate (%) | Cetirizine (DDD) |
| Africa | 15 | 250 | 1.2 | 6 | 25 | 10 | 3 |
| Asia | 20 | 350 | 1.8 | 4.5 | 30 | 15 | 5 |
| Europe | 45 | 220 | 0.8 | 3 | 50 | 55 | 12 |
| N. America | 58 | 180 | 0.7 | 2.5 | 42 | 65 | 14 |
| S. America | 35 | 280 | 1 | 4 | 35 | 40 | 8 |
(Sources: As above) Correlations: UPF-mortality r=0.72 (p less than 0.01); Vit D def-mortality r=0.61.
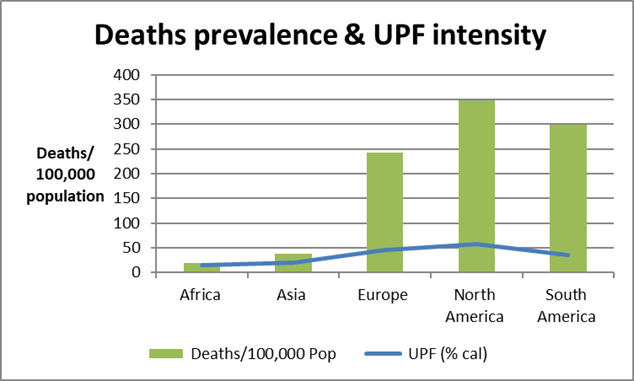
Figure 2: Histogram of Deaths/100,000 by Continent.
Probable Drivers’ Relative Contribution
The above data were checked for VIF (Variance Inflation Factor) is a statistical tool to detect and quantify multi-collinearity, using ChatGPT. The analysis showed the relative contribution of the 5 different related factors in mortality variation across continents as below.
A caution is that the 5 observations and 6 predictors these data are preliminary and not certain or final. Shapley R² decomposition - relative % contributions % of explained variance into contributions of each predictor is as below:
- UPF (ultra-processed food index): 23 %
- Fruit/Veg (kg/yr): 21 %
- Spice (kg/yr): 18 %
- Outdoor hours/day: 16 %
- Vit D deficiency (%): 12 %
- Flu shot rate (%): 10 %
The Shapley decomposition suggests (a) UPF share & fruits-vegetable & spice consumption explain the most of the variance (62%) in mortality across the 5 continents, followed by (b) outdoor hours (78% total of 4 factors). Figure 3 depicts the relative importance of the likely drivers.
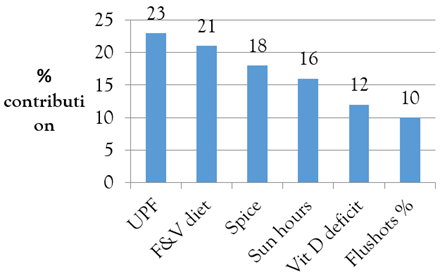
Figure 3: Mortality & lifestyle factors relation.
Discussion
This review interprets results through the lens of innate immunity decline, emphasizing Western diet and lifestyle contributions to COVID-19 disparities. High mortality in North America/Europe (242-349/100,000) versus Asia/Africa (19-38/100,000) aligns with biomarker variances: Vit D deficiency (>50% in Europe) impairs macrophage activation and IFN-γ production, key innate defence against SARS-CoV-2 [10,21]. CRP elevations, proxy for inflammation, were 2-3x higher in Western cohorts [18]. Table 3 indicates inverse correlation of vitamin D-level average mortality values by continents.
Western diets, dominated by UPF (45-58 percentage calories in Europe/N. America vs. less than 20% Asia), promote advanced glycation end-products (AGEs) from preservatives/refrigeration, fostering endothelial dysfunction and cytokine storms [8,22]. Low antioxidants (e.g., polyphenols from spices/fruits) exacerbate oxidative stress; India's 2 kg spice/capita correlate inversely with mortality (r=-0.65), as curcumin/ piperine inhibit viral replication [11,29]. Refrigerated packaged foods reduce microbial exposure, weakening microbiome-trained immunity [7,12]. Sedentary indoor lifestyles (2.5 hrs outdoor/day in N. America) compound Vit D shortfalls, linking to 1.5x higher severe outcomes; quarantine amplified this, increasing deficiency by 20 percentage [25,30].
Medication risks: High flu vaccination (65 percentage N. America) may confer cross-protection (OR=0.83 reduced infection) via trained immunity, yet overuse risks antibody-dependent enhancement hypotheses [31]. Antihistamines like cetirizine (14 DDD/1000 in N. America) suppress histamine-mediated antiviral responses, potentially worsening severity in allergic populations [28,32]. Comparisons: Asia's low rates (15 percentage flu shots) align with natural exposure benefits [27].
Multi-factors: Western diets' AGEs (e.g., from high-heat processed meats) bind RAGE receptors, upregulating NF-κB and IL-6, mirroring COVID-19 hyperinflammation [33]. Low fruit/veg (180 kg/yr N. America) depletes quercetin/flavonoids, reducing ACE2 downregulation [34]. Indoor time (greater than 80 percentage daily in offices) halves UVB exposure, dropping 25(OH)D [21,35]. Interventions such as spice-rich diets (e.g., decoctions) and 15-min daily sun, potentially cutting risks 40% [6,36]. Thus, there is rising trend of Ayurveda & other traditional systems of medicine (TSM) globally [37].
Table 5: Similar Studies on Western Diet/Lifestyle and COVID-19 Outcomes.
| Country | Study Title | Main Findings |
| Global (incl. USA, Brazil) [38] | Plant-based diets and cardiovascular/kidney risks | Plant-based diets lower COVID-19 odds by 73%; Western patterns increase severity via inflammation |
| Syria (model) [39] | Western diet increases COVID-19 severity in hamsters | High-fat/sugar diet worsened lung pathology, mirroring human Western trends |
| UK/Italy [40] | Dietary behaviors and incident COVID-19 | Unhealthy Western diets (high processed) raised infection risk (OR=1.45); plant-based inverse |
| Global [41] | Relation of Dietary Factors with COVID-19 Rates | Pulses/ beans consumption reduced infection and mortality, fruits and sugary beverages increased it |
| Global [42] | Relationship between Mustard Import and COVID-19 Deaths: Globally | Mustard/spice consumption negatively correlated with deaths across 163 countries |
These studies echo patterns: Western UPF/sedentary factors elevate risks via inflammation/Vit D deficits, akin to our r=0.72 UPF-mortality link [22]. Similarity of these findings with other studies globally is indicated in Table 5.
Conclusion
Western diets and lifestyles significantly undermine innate immunity, driving higher COVID-19 burdens in affected regions. Prioritizing fresh, spice-rich foods and outdoor activity could mitigate the future risks.
Abbreviations
COVID-19: Coronavirus Disease 2019
WHO: World Health Organization
Vit D: Vitamin D
UPF: Ultra-Processed Foods
AGEs: Advanced Glycation End-Products
Declarations
Acknowledgements
We acknowledge the support of FRLHT organization heads for moral support and International Journal of Biomedical and Clinical Research editors for pursuing this. We thank Dr. Eva Kuennemann, MVS pharma, GMBH for her insightful comments. No financial support was sought or received for this desk research.
Conflict of Interest
The authors declare no conflicts of interest.
References
- World Health Organization. (2023). WHO COVID-19 Dashboard. Geneva: WHO.
Publisher | Google Scholor - Chinnaswamy, S. (2021). SARS‐CoV‐2 infection in India bucks the trend: Trained innate immunity? American Journal of Human Biology, 33(6):e23504.
Publisher | Google Scholor - Kumar, P., Chander, B. (2020). COVID 19 mortality: Probable role of microbiome to explain disparity. Medical Hypotheses, 144:110209.
Publisher | Google Scholor - Ghate, U., Kulkarni, H. (2021). Polyphenols, spices and vegetarian diet for immunity and anti-inflammatory drug design. In Zepka et al. (eds.) Bioactive Compounds Biosynthesis, Characterization and Applications, 63-76.
Publisher | Google Scholor - Elsayed, Y., Khan, N. A. (2020). Immunity-boosting spices and the novel coronavirus. ACS Chemical Neuroscience, 11(12):1696-1698.
Publisher | Google Scholor - Kulkarni H, Ghate U. (2025). Ayurveda and Herbs as “Fusion Medicines”: Alternatives or Adjuvants to Address Antimicrobial Resistance-A Review. Int J Biomed Clin Res. 3(3):1-7.
Publisher | Google Scholor - Aggarwal, B. B., Shishodia, S. (2006). Molecular targets of dietary agents for prevention and therapy of cancer. Biochemical Pharmacology, 71(10):1397-1421.
Publisher | Google Scholor - Chatterjee, B., Karandikar, R. L., Mande, S. C. (2020). The mortality due to COVID-19 in different nations is associated with the demographic character of nations and the prevalence of autoimmunity. MedRxiv.
Publisher | Google Scholor - Florindo, H. F., Kleiner, R., Vaskovich-Koubi, D., Acúrcio, R. C., Carreira, B., et al. (2020). Immune-mediated approaches against COVID-19. Nature Nanotechnology, 15(8):630-645.
Publisher | Google Scholor - Griffin, G., Hewison, M., Hopkin, J., Kenny, R., Quinton, R., et al. (2020). Vitamin D and COVID-19: evidence and recommendations for supplementation. Royal Society Open Science, 7(12):201912.
Publisher | Google Scholor - Ghate U, Kulkarni H. (2022). Packed Foods Related to COVID-19. J Ecol Nat Reso, 6(4):309.
Publisher | Google Scholor - Ghate, U., Kulkarni, H. (2023). Spices, unpacked diet, bio actives and immunity: Indian health & pandemic. European Journal of Science, Innovation and Technology. 3(3):422-440.
Publisher | Google Scholor - Ghate U, Kulkarni H. (2023) Plant based diet for better immunity, elderly health and environment: Indian insights. Eur J Sci Innov Technol.;4(1):1-12.
Publisher | Google Scholor - Bray, F., Ferlay, J., Soerjomataram, I., Siegel, R. L., Torre, L. A., et al. (2018). Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: A Cancer Journal for Clinicians, 68(6):394-424.
Publisher | Google Scholor - Wang Y, Liu B, Han H, Hu Y, Zhu L, et al. (2023) Associations between plant-based dietary patterns and risks of type 2 diabetes, cardiovascular disease, cancer, and mortality - a systematic review and meta-analysis. Nutr J., 22(1):46.
Publisher | Google Scholor - Our World in Data. (2023). Cumulative confirmed COVID-19 cases and deaths. Oxford: OWID.
Publisher | Google Scholor - OECD/FAO. (2023). Agricultural Outlook 2023-2032. Paris: OECD.
Publisher | Google Scholor - Amrein, K., Scherkl, M., Hoffmann, M., Neuwersch-Sommeregger, S., Köstenberger, M., et al. (2020). Vitamin D deficiency 2.0: an update on the current status worldwide. European Journal of Clinical Nutrition, 74(11):1498-1513.
Publisher | Google Scholor - Eurostat. (2022). Fruit and vegetable consumption in Europe. Luxembourg: Eurostat.
Publisher | Google Scholor - Worldometer. (2023). COVID-19 Statistics. Dover: Worldometer.
Publisher | Google Scholor - Cui, A., Zhang, T., Xiao, P., Fan, Z., Wang, H., et al. (2023). Global and regional prevalence of vitamin D deficiency in population-based studies from 2000 to 2022: A pooled analysis of 7.9 million participants. Frontiers in Nutrition, 10:1070808.
Publisher | Google Scholor - Hall, K. D., Ayuketah, A., Brychta, R., Cai, H., Cassimatis, T., et al. (2019). Ultra-processed diets cause excess calorie intake and weight gain: an inpatient randomized controlled trial of ad libitum food intake. Cell Metabolism, 30(1):67-77.
Publisher | Google Scholor - World Population Review. Vegetable Consumption by Country 2025.
Publisher | Google Scholor - Lee, S. H. (2022). Adults meeting fruit and vegetable intake recommendations-United States, 2019. Morbidity and Mortality Weekly Report, 71.
Publisher | Google Scholor - Wikipedia. List of cities by sunshine duration.
Publisher | Google Scholor - Current Results. Sunniest Places and Countries in the World.
Publisher | Google Scholor - World Population Review. Flu Vaccination Rates by Country 2025.
Publisher | Google Scholor - Urrutia-Pereira, M., Chong-Neto, H. J., Maesano, I. A., Ansotegui, I. J., Caraballo, L., et al. (2022). Environmental contributions to the interactions of COVID-19 and asthma: A secondary publication and update. World Allergy Organization Journal, 15(9):100686.
Publisher | Google Scholor - Negi, S., Bhatt, S., Bala, L. (2021). Prevention of SARS-CoV-2 Infection with Antioxidants and Anti-inflammatory Action of Indian Spices: Light at the End of the Tunnel. Journal of Clinical & Diagnostic Research, 15(8).
Publisher | Google Scholor - Pedersen, E. S., Mallet, M. C., Lam, Y. T., Bellu, S., Cizeau, I., et al. (2021). COVID-19 vaccinations: perceptions and behaviours in people with primary ciliary dyskinesia. Vaccines, 9(12):1496.
Publisher | Google Scholor - Trieu MC, Bansal A, Sævik M, Ljostveit S, Jul-Larsen Å, et al. (2025). Effects of repeated influenza vaccination and infection on durable seroprotection in healthcare workers. NPJ Vaccines. 10(1):213.
Publisher | Google Scholor - Kong W, Dong Y, Yi S, Mo W, Yang H. (2024). High-risks drug adverse events associated with Cetirizine and Loratadine for the treatment of allergic diseases: A retrospective pharmacovigilance study based on the FDA adverse event reporting system database. Clin Transl Allergy. 14(9):e12392.
Publisher | Google Scholor - Zhou, L., Li, H., Zhang, S., Yang, H., Ma, Y., et al. (2023). Impact of ultra-processed food intake on the risk of COVID-19: a prospective cohort study. European Journal of Nutrition, 62(1):275-287.
Publisher | Google Scholor - Ghate, U. Kulkarni, H. (2023). Quercetin-herbal Bioactive Nanotechnology for Osteoarthritis and Elderly Health. Brazilian Journal of Development, 9(12):31772-31783.
Publisher | Google Scholor - Ghate, U. Kulkarni, H. (2023). Quercetin-herbal Bioactive Nanotechnology for Osteoarthritis and Elderly Health. Brazilian Journal of Development, 9(12):31772-31783.
Publisher | Google Scholor - Kunnumakkara, A. B., Sailo, B. L., Banik, K., Harsha, C., Prasad, S., et al. (2018). Chronic diseases, inflammation, and spices: how are they linked? Journal of Translational Medicine, 16(1):14.
Publisher | Google Scholor - Ghate U, Wele A. (2022). Globalization of AYUSH Products: Status, Challenges and Suggestions for Growth. Traditional Medicine Review, 1(2):21-34.
Publisher | Google Scholor - Kim, H., Caulfield, L. E., Garcia-Larsen, V., Steffen, L. M., Coresh, J., et al. (2019). Plant‐ based diets are associated with a lower risk of incident cardiovascular disease, cardiovascular disease mortality, and all-cause mortality in a general population of middle-aged adults. Journal of the American Heart Association, 8(16):e012865.
Publisher | Google Scholor - Port JR, Adney DR, Schwarz B, Schulz JE, Sturdevant DE, et al. (20210. Western diet increases COVID-19 disease severity in the Syrian hamster. bioRxiv
Publisher | Google Scholor - Vu TT, Rydland KJ, Achenbach CJ, Van Horn L, Cornelis MC. (2021). Dietary Behaviors and Incident COVID-19 in the UK Biobank. Nutrients. 13(6):2114.
Publisher | Google Scholor - Abdulah DM, Hassan AB. (2020). Relation of Dietary Factors with Infection and Mortality Rates of COVID-19 across the World. J Nutr Health Aging. 24(9):1011-1018.
Publisher | Google Scholor - Zhan, G., Yang, F., Zhang, L., Wang, H. (2022, October). The Relationship between Mustard Import and COVID-19 Deaths: A Workflow with Cross-Country Text Mining. In Healthcare. 10(10):2071.
Publisher | Google Scholor























