

Case Report
Comprehensive Dental Rehabilitation Under General Anaesthesia in a 28-Year-Old Adult Male with Autism Spectrum Disorder: A Case Report and Review of Behavioural and Clinical Management Strategies
- Chirag Chamria
- Jemmie Joy Alexander *
Oral & Maxillofacial Surgeon, MDS Royal Dental Clinics, Mumbai, India.
*Corresponding Author: Jemmie Joy Alexander, BDS Oral & Maxillofacial Surgeon, MDS Royal Dental Clinics, Mumbai, India.
Citation: Chamria C., Jemmie J. Alexander. (2026). Comprehensive Dental Rehabilitation Under General Anaesthesia in a 28-Year-Old Adult Male with Autism Spectrum Disorder: A Case Report and Review of Behavioural and Clinical Management Strategies, Clinical Case Reports and Studies, BioRes Scientia Publishers. 12(1):1-5. DOI: 10.59657/2837-2565.brs.26.295
Copyright: © 2026 Jemmie Joy Alexander, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: December 02, 2025 | Accepted: December 24, 2025 | Published: January 09, 2026
Abstract
Background: Adults with autism spectrum disorder (ASD) often face substantial barriers in receiving routine dental care, resulting in unmet oral health needs, untreated caries, and episodic dental pain. Literature reports increased dental anxiety, sensory hypersensitivity, limited tolerance to clinical procedures, and dependence on caregivers, especially in males with severe behavioural expression.
Case Presentation: A 28-year-old adult male with ASD residing in Mumbai presented with severe dental pain and inability to cooperate during examination. Behavioural challenges included hyperactivity, non-verbal communication patterns, and inability to tolerate intraoral procedures. Based on risk assessment and predicted lack of cooperation, treatment was planned under general anaesthesia (GA). A full-mouth rehabilitation was executed: Root canal therapy and post placement for the right upper molars, also root canal therapy for right lower first molar, extraction, and immediate implant placement for the left upper and lower first molars, and prefabricated crowns placed intraoperatively. Procedure and recovery were uneventful; patient was discharged two hours post-op. At one-week review, the family reported no pain or complications. At a six-month teleconsultation, the patient was asymptomatic and functioning well.
Conclusion: This case demonstrates the importance of providing timely and comprehensive dental treatment under GA for adults with ASD who cannot cooperate with conventional care. Early intervention, caregiver collaboration, and appropriate behaviour-based planning can prevent progression to dental emergencies. The report reinforces the message that general practitioners and specialists should confidently manage special-needs patients with structured protocols.
Keywords: autism spectrum disorder; adult dentistry; general anaesthesia; behaviour management; special care dentistry; full-mouth rehabilitation; implants; prefabricated crowns
Introduction
Autism spectrum disorder (ASD) is associated with distinctive behavioural, sensory, and communication characteristics that significantly influence dental care delivery. Adults with ASD, even those with adequate family support, often present with elevated dental fear, reduced attendance, untreated caries, and reliance on emergency-driven treatment (Blomqvist et al., 2015). Many studies show that adult autistic individuals exhibit heightened sensory reactivity, difficulty adapting to change, and poor tolerance for tactile, auditory, and visual stimuli encountered in the dental setting (Limeres-Posse et al., 2014; Chandrashekhar et al., 2018).
Barriers include communication challenges, behavioural dysregulation, limited desensitisation, and inadequate training of dental practitioners (Jones et al., 2024; Prynda et al., 2024). For patients who cannot tolerate routine care, treatment under general anaesthesia (GA) remains evidence-based and safe (Son et al., 2024; Czornobay et al., 2018). This case presents the comprehensive management of a 28-year-old autistic adult requiring simultaneous restorative, endodontic, and implant procedures.
Case Description
Patient Background
A 28-year-old autistic male residing in Mumbai, living with family and caretakers at a farmhouse in Lonavala, presented with acute dental pain and marked behavioural hyperactivity. He was non-verbal with limited comprehension, highly uncooperative with touch, and unable to sit still for examination. Caregivers reported disturbed sleep due to pain.
Clinical & Radiographic Findings
Although chairside examination was restricted, the patient permitted an OPG radiograph shown in Figure 1a , which revealed pathology involving all four first molars. Findings included:
- #16 – Fractured crown with pain and sensitivity.
- #14 – Deep Caries
- #15, #11, #12 – Proximal Caries
- #26, #36 – Root piece (Figure 2a and 2b)
- #46 – Root canal treated tooth with chronic periapical pathology
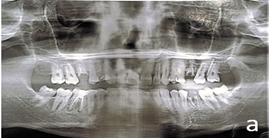
Figure 1a: Before treatment OPG

Figure 1b: After treatment OPG

Figure 2a: Before treatment clinical photograph #36

Figure 2b: Before treatment clinical photograph #26
Behavioural Assessment
Multiple indicators confirmed that conventional treatment would be impossible, including:
- Extreme hyperactivity
- Inability to communicate pain
- Sensory defensiveness
- Zero tolerance to instruments or touch
- High distress in clinical environment
These align with contemporary literature documenting behavioural dysregulation, sensory overload, and dental fear in adults with ASD (Blomqvist 2015; Pastore 2023; Prynda 2024).
Treatment Planning
Given behavioural challenges and multi-quadrant disease, a single-stage, comprehensive care approach under GA was planned, consistent with recommendations for patients with severe ASD (Limeres-Posse et al., 2014; Son et al., 2024).
The plan included:
Oral Prophylaxis
Fillings - #15, #11, #12
Root Canal Therapy - #16, #46, #14 (Figure 3)
Extraction - #26, #36
Implants - #26, #36
Prefab Prosthesis - #14, #16, #26, #36, #46 (Figure 4).

Figure 3: Clinical photograph taken during procedure #14

Figure 4: Immediate postoperative clinical photograph #46
Treatment Under General Anaesthesia
Anaesthetic Protocol
Patient was intubated via the right naso-endotracheal tube. GA was induced and maintained uneventfully.
The procedure lasted approximately 90 minutes.
Intraoperative Workflow
- Oral Prophylaxis
- Fillings - #12
- Root Canal Therapy - #14, #16, #46,
- Extraction - #26, #36
- Implants - #26, #36
- Prefab Prosthesis - #14, #16, #26, #36, #46
- Occlusion adjusted to reduce high contacts, considering the patient's bruxism tendencies common in ASD adults (Prynda 2024).
Recovery
Patient recovered smoothly and was discharged 2 hours post-operatively. Caregivers received instructions on analgesia, soft diet, and implant hygiene.
Follow-Up
1-Week Review (In-Person)
Post operative radiograph was taken in the follow up appointment as shown in ‘Figure 1b’
Family reported:
- No pain
- Good acceptance of food
- No distress or behavioural changes
Clinical evaluation showed:
- Stable healing
- No inflammation
- Good crown retention
6-Month Follow-Up (Virtual Consultation)
Due to difficulty transporting the patient, teleconsultation was used. Caregivers reported:
- No pain or swelling
- Normal eating habits
- Restored comfort and sleep
- No prosthesis-related issues
This aligns with literature supporting tele-dentistry for ASD patients with travel limitations (Floríndezet al., 2024).

Figure 5: 6-month follow-up photograph (clicked during virtual consult)
Discussion
Adults with ASD frequently experience unmet oral health needs due to behavioural challenges, sensory sensitivities, and systemic access barriers (Jones et al., 2024). Dental avoidance is common, often leading to emergency-based care, similar to the present case (Blomqvist 2015). Behavioural manifestations in ASD—hyperactivity, reduced attention, and distress during unfamiliar stimuli—limit tolerance to routine procedures (Czornobay 2018; Pastore 2023).
When non-pharmacologic methods fail or multiple complex procedures are required, GA becomes the safest modality. Evidence shows it results in high caregiver satisfaction, allows comprehensive care, and prevents repeated traumatic encounters (Son et al., 2024).
Given difficulty returning for sit-down appointments, durable options—RCT with posts and prefabricated crowns, and implant-supported rehabilitation—are ideal. Simplification and reduction of future treatment burden are recommended in adults with ASD (Zerman 2022).
The family’s stable support structure significantly contributed to postoperative recovery, aligning with studies showing caregiver-facilitated routines improve outcomes (Floríndez 2024).
The case reinforces that general dentists and specialist should not hesitate to treat ASD adults when a structured approach is used. A combination of:
- Adequate preoperative planning
- Behavioural assessment
- Sensory-friendly interactions
- Use of GA when required
- Long-term follow-through via teleconsultations
can achieve predictable, complication-free outcomes.
This case adds to literature encouraging wider acceptance of ASD patients in mainstream dental practice and underscores the value of GA-supported comprehensive treatment in adults with severe behavioural limitations.
Conclusion
This report highlights the successful rehabilitation of a 28-year-old autistic adult using a single-stage same day dentistry approach, comprehensive approach under GA. The outcome demonstrates that with careful planning, empathetic caregiver collaboration, and appropriate behavioural considerations, dentists can deliver effective and humane care even for non-cooperative ASD patients. The case supports broader training and confidence among dental professionals to treat individuals with special needs.
Declarations
Note
All figures [Figure 1 to 5] are original clinical images captured during the treatment of the patient described in this case report.
Conflict of Interest
The authors report no conflict of interest
Ethical Statement
Written informed consent for treatment and publication of this case report, including clinical details and images, was obtained from the patient’s legal guardian. All clinical images (Figures 1–5) are original and were obtained during the course of treatment of the patient.
References
- Blomqvist, M., Bejerot, S., & Dahllöf, G. (2015). Oral health, dental anxiety, and dental behavior in intellectually able adults with autism spectrum disorder. BMC Oral Health.
Publisher | Google Scholor - Shapira, J., et al. (1989). Oral health status and dental needs of an autistic population. Special Care in Dentistry.
Publisher | Google Scholor - Jones, R., et al. (2024). Barriers to oral health care for autistic individuals: A scoping review.
Publisher | Google Scholor - Pastore, L., et al. (2023). Behavioral guidance strategies for dental treatment in ASD patients.
Publisher | Google Scholor - Prynda, M., et al. (2024). Dental adaptation strategies for autistic individuals: Systematic review.
Publisher | Google Scholor - Chandrashekhar, S., et al. (2018). Management of autistic patients in dental office: A clinical update.
Publisher | Google Scholor - Czornobay, T., et al. (2018). Autism spectrum disorder: A review and dental management.
Publisher | Google Scholor - Limeres-Posse, J., et al. (n.d.). Behavioral aspects of patients with autism during dental care.
Publisher | Google Scholor - Son, J., et al. (2024). Ten-year comparative analysis of behavior management techniques in dental patients with ASD.
Publisher | Google Scholor - Floríndez, J., et al. (2024). Oral care interventions for autistic individuals: Systematic review.
Publisher | Google Scholor - Zerman, N., et al. (2022). Dental care management and prevention strategies in ASD.
Publisher | Google Scholor - Autism Speaks. (n.d.). Dental toolkit for ASD patients.
Publisher | Google Scholor - Fallea, A., et al. (2024). Oral health-related quality of life in autism spectrum disorder.
Publisher | Google Scholor























