

Research Article
Comparison of Intrathecal Bupivacaine and Dexamethasone with Intrathecal Bupivacaine and Fentanyl for Lower Limb Surgeries
Department of Anaesthesia, Christian Medical College and Hospital, Ludhiana, Punjab.
*Corresponding Author: Dr. Valsaamma Abraham,Department of Anaesthesia, Christian Medical College and Hospital, Ludhiana, Punjab.
Citation: Kaur. M, Abraham. V, Kaur. N. (2025). Comparison of Intrathecal Bupivacaine and Dexamethasone with Intrathecal Bupivacaine and Fentanyl for Lower Limb Surgeries, International Journal of Medical Case Reports and Reviews, BioRes Scientia Publishers. 5(3):1-7. DOI: 10.59657/2837-8172.brs.25.081
Copyright: © 2025 Dr. Valsaamma Abraham, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: April 11, 2025 | Accepted: April 22, 2025 | Published: April 24, 2025
Abstract
Spinal anaesthesia is the most consistent block for lower limb surgeries. Spinal anaesthesia avoids the risk of general anaesthesia such as aspiration of gastric contents and difficulty with airway management. For lower limb orthopedic surgery, spinal anesthesia is a simple, affordable, and ideal approach because it offers a quick and efficient sensory and motor blockade, reduces the stress response, and lowers the risk of thromboembolic events.
Bupivacaine is appropriate for procedures lasting for 90 -120 minutes. Therefore, many additives such as opioids like fentanyl are added to local anaesthetics that prolongs the effect of local anaesthetic. Recent studies reported the effects of corticosteroids in quality and quantity of sensory block in peripheral nerves. Dexamethasone relieves pain by reducing inflammation and blocking transmission of nociceptive C fibers and by suppressing ectopic neural discharges. Intrathecal dexamethasone as an adjuvant to spinal bupivacaine proves to be effective as it prolongs the duration of analgesia, stable haemodynamic profile with minimal side effects.
Aims and Objectives: To compare the efficacy of intrathecal bupivacaine and dexamethasone with intrathecal bupivacaine and fentanyl.
Materials and Methods: This study was a double blinded prospective randomised study conducted on 60 patients of either sex, aged between 18- 55 years at the Department of Anaesthesia, Christian Medical College & Hospital, Ludhiana. Group I received 0.5% hyperbaric bupivacaine with dexamethasone, while Group II received 0.5% hyperbaric bupivacaine with fentanyl and normal saline. Vital signs, duration of analgesia, duration of sensory and motor block was monitored intraoperatively. Vitals were monitored in the post-operative period along with the pain assessment using VAS Scale.
Conclusion: Our study showed that intrathecal dexamethasone and intrathecal fentanyl maintains a good hemodynamic profile but the mean duration of analgesia and mean duration of sensory and motor block was better in intrathecal dexamethasone group than intrathecal fentayl group. The post-operative pain control in dexamethasone group was better. Overall, intrathecal dexamethasone was better than intrathecal fentanyl in lower limb surgeries.
Keywords: dexamethasone; fentanyl; bupivacaine; lower limb surgeries
Introduction
One of the most used anesthetic techniques for lower limb surgery is spinal anesthesia [1]. For lower limb orthopedic surgery, spinal anesthesia is a simple, affordable, and ideal approach because it offers a quick and efficient sensory and motor blockade, reduces the stress response, and lowers the risk of thromboembolic events [2]. A few benefits of this approach are that the patient remains awake during the procedure; it acts quickly, has a low failure rate, uses a modest dosage of the medication, produces acceptable motor and sensory blocks, and is reasonably priced [3]. The comparison between intrathecal bupivacaine and dexamethasone versus intrathecal bupivacaine and fentanyl is of significant clinical interest, as both combinations are commonly used in spinal anesthesia and pain management but have different mechanisms of action. Dexamethasone is a potent corticosteroid with anti-inflammatory properties, which could potentially enhance the duration and effectiveness of bupivacaine, a local anesthetic, by reducing inflammation at the site of nerve blockade [4]. On the other hand, fentanyl, an opioid, is known for its powerful analgesic effects and may provide rapid and effective pain relief when combined with bupivacaine. Understanding the comparative efficacy of these two combinations is crucial in determining the most optimal and long-lasting pain management approach for patients undergoing spinal procedures. Additionally, investigating the side effects of these drug combinations is essential for ensuring patient safety [5]. While dexamethasone has relatively few systemic side effects, fentanyl may lead to more significant concerns such as respiratory depression and sedation [6].
By systematically comparing the efficacy and side effects of these two combinations, this study aims to provide valuable insights into their relative benefits and risks, ultimately guiding clinicians toward the most effective and safest pain management strategies.
Material and Methods
Study Design: This research used a double-blind, randomized design.
Source of data: Sixty patients, aged 18 to 55, who were undergoing elective lower limb surgery under spinal anesthesia for two to three hours were studied at the anesthesia department of Christian Medical College & Hospital in Ludhiana. Informed consent was obtained after institutional research committee and ethics committee clearance. Every patient underwent a detailed history, proper physical examination, and a review of pertinent investigations. A computer-generated sequence was used to randomly split the patients into two groups of thirty each. Patients in Group I received 12.5 mg (2.5 ml) of 0.5% hyperbaric bupivacaine and 4 mg (1 ml) of dexamethasone while 12.5 mg (2.5 ml) of 0.5% hyperbaric bupivacaine, 25 mcg (0.5 ml) of fentanyl, and 0.5 ml of NS was administered to Group II patients. Total volume of 3.5 ml in each group.
Inclusion criteria
ASA I and II
Either sex
Adult (18–55 years old)
A two to three-hour elective lower limb surgery performed under spinal anesthesia.
Exclusion criteria
Patients with a substantial neurological impairment.
Operations on spinal columns
Extended history of using steroids.
Allergic to local anesthesia.
A fentanyl allergy.
Statistical Analysis
To determine the relationship between the groups category variables, the chi square test will be used. Mann-Whitney test or independent t test The U test was used to determine how two groups' continuous outcomes differed from one another. P values less than 0.05 was regarded as significant. SPSS version 28.0 was used for all statistical analysis.
Results
In our study in Group I, 30.0% of cases were female, while in Group II, 23.3% were female. Conversely, males constituted 70.0% and 76.7% of cases in Group I and Group II, respectively and both groups were comparable (p value 0.559). The mean age in Group I was 41.83 ± 11.02 years, while in Group II, it was 42.00 ± 12.96 years. In Group I, the mean duration of the surgery was 134.00 minutes, with a standard deviation (SD) of 14.29 minutes. In Group II, the mean duration was slightly higher at 136.33 minutes, with a SD of 13.77 minutes. The t-test resulted in a t-value of -0.644 and a p-value of 0.522.
Onset of motor and sensory block
The onset of sensory block, in Group I, the mean onset time was 11.13 minutes, with a standard deviation (SD) of 1.48 minutes. In Group II, the mean onset time was slightly lower at 10.47 minutes, with a SD of 1.20 minutes. The Z-score for this comparison was 1.920, resulting in a p-value of 0.060, which was not statistically significant.
Regarding the onset of motor block, in Group I, the mean onset time was 11.20 minutes, with a standard deviation (SD) of 1.54 minutes. In Group II, the mean onset time was slightly higher at 11.47 minutes, with a SD of 1.25 minutes. The Z-score for this comparison was -0.736, resulting in a p-value of 0.465, which was not statistically significant. The mean time taken to achieve maximum level of sensory block (minutes) in group 1 was 20.37±2.86 and in group II was 17.53±2.24. On comparison there was statistically significant difference in between the two groups (p=0.001).
The duration of sensory and motor blocks between two groups receiving different intrathecal combinations. In Group I (Intrathecal Bupivacaine and Dexamethasone), the mean duration of the sensory block was 283.33 minutes with a standard deviation of 12.13 minutes, and the mean duration of the motor block was 215.67 minutes with a standard deviation of 9.37 minutes. In contrast, Group II (Intrathecal Bupivacaine and Fentanyl) exhibited significantly shorter durations for both blocks. The mean sensory block duration in Group II was 194.33 minutes with a standard deviation of 11.35 minutes, and the motor block lasted an average of 158.00 minutes with a standard deviation of 12.13 minutes. These results show that Group I provided a longer duration of both sensory and motor blocks compared to Group II, with the mean differences being statistically significant.
In our study mean time taken to achieve max level of sensory block (minutes) in group 1 was 20.37±2.86mins and in group II was 17.53±2.24mins.
The table presents data comparing the occurrence of various side effects between Group I, and Group II. In both groups, the majority of participants did not experience nausea, vomiting, hypotension, bradycardia, tinnitus, blurred vision, or allergic reactions to the drug. For nausea, 2 patients in group I had nausea while 4 patients in group II had nausea (p=0.671). Similarly, 2 patients in group I had vomiting and 4 patients in group II had vomiting and there were no statistically significant differences between the two groups (p=0.671)
In our study duration of analgesia (hours) in group I was 7.17±4.54 and in group II was 3.03±2.04. On comparison there was statistically significant difference in between the two groups (P=0.001).
In our study, mean values and standard deviations (SD) of pain intensity scores assessed using the Visual Analog Scale (VAS) at various post-operative period time intervals for Group I, which received intrathecal bupivacaine and dexamethasone and Group II, which received intrathecal bupivacaine and fentanyl.
Table 1: Demographic Parameter of Patients
| Group I | Group II | T | p-value | |||
| Mean | SD | Mean | SD | |||
| AGE | 41.37 | 11.02 | 42 | 12.96 | -0.204 | 0.839 |
| HEIGHT IN METER | 1.68 | 0.08 | 1.69 | 0.08 | -0.746 | 0.459 |
| WEIGHT(Kg) | 69.63 | 9.17 | 74.53 | 11.78 | -1.798 | 0.077 |
| BMI | 24.86 | 3.49 | 26.19 | 4.97 | -1.205 | 0.233 |
Table 2: Comparison of adverse events in between the two groups
| Group I | Group I | Group II | Group II | Total | Chi- square value | p- value | |
| Nausea | 2 | 6.70% | 4 | 13.30% | 6 | 0.671 | |
| Vomiting | 2 | 6.70% | 4 | 13.30% | 6 | 0.671 | |
| Hypotension | 0 | 0.00% | 0 | 0.00% | 0 | ||
| Bradycardia | 0 | 0.00% | 0 | 0.00% | 0 | ||
| Tinnitus | 0 | 0.00% | 0 | 0.00% | 0 | ||
| Blurred Vision | 0 | 0.00% | 0 | 0.00% | 0 | ||
| Allergic Rection to Drug | 0 | 0.00% | 0 | 0.00% | 0 | ||
| Total | 100.00% | 30 | 100.00% | 60 |
Discussion
In our study the comparison of mean age between Group I, which received intrathecal bupivacaine and dexamethasone and in Group II, which received intrathecal bupivacaine and fentanyl. The mean age in Group I was 41.83 years with a standard deviation (SD) of 11.02 years, while in Group II, it was 42.00 years with a SD of 12.96 years. The t-value obtained was -0.204, with a corresponding p-value of 0.839 showing both the groups were comparable.It was comparable with the study by Fayyaz et al in-group BD (Bupivacaine with Dexamethasone), there were 9 (30%) patients of age range 18-25 years, 10 (33.33%) between 26 to 30 years, 5 (16.66%) of age range 31-35 years and 6 (20%) were between the 36-40 years range. In group BS (Bupivacaine), (Control), there were 12 (40%) patients of age range 18-25 years, 8 (26.66%) between 26 to 30 years, 6 (20%) of age range 31-35 years and 4 (13.33%) were between the 36-40 years range [7].
Duration of surgery
In our study In Group I, the mean duration of the surgery was 134.00 minutes, with a standard deviation (SD) of 14.29 minutes. In Group II, the mean duration was slightly higher at 136.33 minutes, with a SD of 13.77 minutes. The p-value of 0.522 indicates no statistically significant difference in the mean duration of the surgery between the two groups, indicating both the groups were comparable. Our results were comparable with a study conducted by Kaur H et al. [4]. the duration of surgery in the three groups was found to be 86.14 (±15.02) minutes in group I, 88.29 (±13.39) minutes in group II and in group III the mean surgical duration was 86.20±13.45 minutes which was statistically insignificant (p = 0.211). In both group the hemodynamic parameters and oxygen saturation during lower limb surgeries, the findings revealed no significant differences in heart rate, systolic and diastolic blood pressure, mean arterial pressure, or oxygen saturation between the two groups throughout the 180-minute observation period intraoperatively. Both groups showed similar baseline levels and variations in these parameters, with slight fluctuations attributed to the effects of dexamethasone and sympathetic blockade from the fentanyl. Ultimately, both drug combinations provided hemodynamic stability, indicating their efficacy in maintaining physiological parameters during surgery.
Onset of motor and sensory block
In our study onset of sensory block, in Group I, the mean onset time was 11.13 minutes, with a standard deviation (SD) of 1.48 minutes. In Group II, the mean onset time was slightly lower at 10.47 minutes, with a SD of 1.20 minutes. The Z-score for this comparison was 1.920, resulting in a p-value of 0.060, showing both the groups were comparable. Regarding the onset of motor block, in Group I, the mean onset time was 11.20 minutes, with a standard deviation (SD) of 1.54 minutes. In Group II, the mean onset time was slightly higher at 11.47 minutes, with a SD of 1.25 minutes. The Z-score for this comparison was -0.736, resulting in a p-value of 0.465(insignificant), showing both the groups were comparable.
Compare to study conducted by Kaur H et al [4]. conducted a study on patients received an intrathecal injection of hyperbaric bupivacaine (12.5 mg) with 4 mg of dexamethasone in group I, hyperbaric bupivacaine (12.5 mg) with 25 ug fentanyl with 0.5 ml of normal saline in group II and hyperbaric bupivacaine (12.5 mg) with normal saline (1 ml) in group III. The onset of sensory and motor block was comparable among all the groups. In a study conducted by Bani Hasham et al 8 The onset time of sensory block was 11.2±2.0 minutes for the case group and 10.9±1.8 minutes for the control Group (P=0.57).
Duration of sensory and motor block
In our study, results showed significant differences between the two groups in terms of both sensory and motor block durations. Group I exhibited substantially longer durations of sensory block (283.33 mins) and motor block (215.67 mins) compared to Group II, which had shorter durations sensory block (194.33 mins), motor block (158.00 mins). Statistical analysis confirmed these differences to be highly significant (p < 0>A study by Fayyaz et al [7]. compared the mean duration of analgesia with intrathecal bupivacaine alone versus intrathecal bupivacaine plus dexamethasone, for elective caesarean section. They concluded that hyperbaric bupivacaine and dexamethasone provided 391±25.51 minutes of analgesia as compared to hyperbaric bupivacaine alone 179.43±23.32 minutes which was statistically significant. In study conducted by Alarasan AK, 20169 duration of sensory and motor block was significantly prolonged in dexamethasone group (366 ± 28.11 and 337.33 ± 28.75) minutes compared to control group (242.66 ± 26.38 and 213 ± 26.80) minutes.
Time taken to achieve maximum level of sensory block
In our study mean time taken to achieve max level of sensory block (minutes) in group 1 was 20.37±2.86mins and in group II was 17.53±2.24mins. On comparison there was statistically significant difference in between the two groups (P=0.001). Similar results were seen in this study conducted by Esmat et al10 where time taken to achieve peak sensory block was significantly higher.
Intrathecal dexamethasone as an analgesic could be explained by influencing prostaglandin production. Dexamethasone relieves pain through reducing inflammation and blocking of nociceptive C fibers transmission and by suppressing neural ectopic discharges.
Duration of analgesia
In our study duration of analgesia (hours) in group I was 7.17±4.54 and in group II was 3.03±2.04. On comparison there was statistically significant difference in between the two groups (P=0.001).
A study conducted by Kaur H et al [4]. compared the mean duration of analgesia was 311.43±13.59 min with intrathecal bupivacaine and dexamethasone versus 197.86±86 min in intrathecal bupivacaine with fentanyl and 115.29 min in intrathecal bupivacaine with normal saline and was statistically significant, p=<0>A study by Fayyaz etal [7]. compared the mean duration of analgesia with intrathecal bupivacaine alone versus intrathecal bupivacaine plus dexamethasone, for elective caesarean section. They concluded that hyperbaric bupivacaine and dexamethasone provided 391±25.51 minutes of analgesia as compared to hyperbaric bupivacaine alone 179.43±23.32 minutes which was statistically significant.
VAS score
In our study mean values and standard deviations (SD) of pain intensity scores assessed using the Visual Analog Scale (VAS) at various post-operative period time intervals for Group I, which received intrathecal bupivacaine and dexamethasone and Group II, which received intrathecal bupivacaine and fentanyl.
During the early hours post-operative period (1 to 4 hours), Group II consistently exhibits significantly higher VAS scores compared to Group I, indicating higher perceived pain levels in the fentanyl group during this period which was statistically significant, p=0.001
However, from 6 to 24 hours post-operative period, the differences in VAS scores between the groups were not statistically significant (p > 0.05), suggesting similar pain outcomes between the two groups during these later hours.
In study conducted by Alarasan AK et al9 VAS score in the postoperative period was higher (P < 0>Adverse effects
In our study, 6.7% of group I and 13.3% of group II had nausea. Nevertheless, the difference (p=0.671) does not reach statistical significance. 13.3% of group II and 6.7% of group I had vomiting. There was no statistically significant difference between the two groups. Similar results were reported in study conducted by Kaur H et al4 in group III, two patients had nausea/vomiting, one patient each had bradycardia, hypotension and shivering.
Our study concluded that
1. Both Intrathecal dexamethasone and fentanyl had equally good control of
hemodynamic variables.
2. Intrathecal dexamethasone provided a prolonged duration of analgesia as
compared to intrathecal fentanyl
3. Intrathecal dexamethasone showed prolonged duration of sensory and motor
block
4. Mean time taken to reach maximum level of sensory block was more in
dexamethasone group.
5. Pain control in postoperative period was better in the intrathecal dexamethasone
Group compared to fentanyl
In Conclusion our study showed that intrathecal dexamethasone and intrathecal fentanyl maintains a good hemodynamic profile but the mean duration of analgesia and mean duration of sensory and motor block was better in intrathecal dexamethasone group than intrathecal fentayl group. The post-operative pain control in dexamethasone group was better. Overall, intrathecal dexamethasone was better than intrathecal fentanyl in lower limb surgeries.
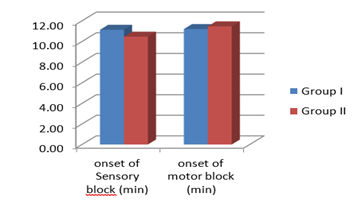
Figure 1: Comparison of the mean onset of sensory block and motor block (in minutes) between the two groups
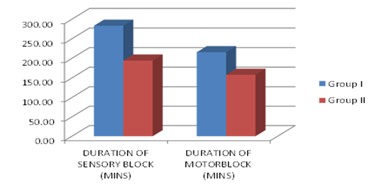
Figure 2: Comparison of the duration of sensory block and motor block (min) in both the groups
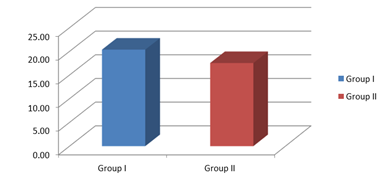
Figure 3: Mean time taken to achieve maximum level of sensory block in both the groups
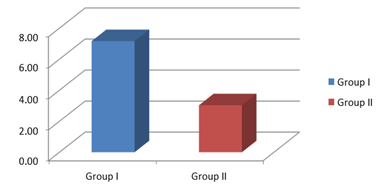
Figure 4: Comparison of the duration of analgesia (in hours) between Group I and Group II.
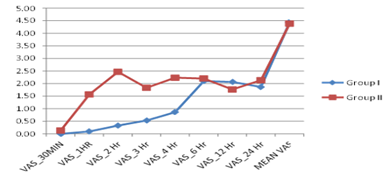
Figure 5: Comparison of mean values and standard deviations (SD) of pain intensity scores measured using the Visual Analog Scale (VAS) at different time points post-operative period in between the two groups
Declarations
Acknowledgements: None
Conflict of Interest: We declared that we do not have any conflict of interest in this manuscript
Author Contribution: Dr Manveet Kaur: Substantial contributions to the conception or design of the work or the acquisition, analysis, or interpretation of data for the work; Drafting the work or reviewing it critically for important intellectual content.
Final approval of the version to be published Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Dr Valsaamma Abraham: Substantial contributions to the conception or design of the work or the acquisition, analysis, or interpretation of data for the work; Drafting the work or reviewing it critically for important intellectual content; Final approval of the version to be published; Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved
Dr Narjeet Kaur: Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; Drafting the work or reviewing it critically for important intellectual content; Final approval of the version to be published; Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved
References
- Ahmed MM, Khaliq Ahmed Md, Alugolu M, Kumar JN. (2025). Enhancing Spinal Anesthesia for Lower Limb Surgeries: A Comparative Study of Intrathecal Midazolam and Hyperbaric Bupivacaine. J Neonatal Surg, 14(8S):6-10.
Publisher | Google Scholor - Mazy A, Ghanem MA, Abd Elatif MS, Basyoni YE. (2019). Spinal anesthesia for lengthy lower limb orthopedic surgeries: dexmedetomidine plus fentanyl versus dexmedetomidine. Ain-Shams Journal of Anesthesiology, 18:11(1).
Publisher | Google Scholor - Paliwal N, Kokate MV, Deshpande NA, Khan IA. (2024). Spinal Anaesthesia Using Hypobaric Drugs: A Review of Current Evidence. Cureus. 16(3):e56069.
Publisher | Google Scholor - Kaur, H., Misra, R., Mittal, S., & Sidhu, G. A. S. (2021). Prospective randomized control trial comparing the effect of dexamethasone versus fentanyl as adjuvants
Publisher | Google Scholor - Nasiri A, Abutorabi SM, Sane S. (2024). Intrathecal dexamethasone-bupivacaine combination with bupivacaine alone in spinal anesthesia for cesarean delivery. Caspian J Intern Med. 15(3):414-420.
Publisher | Google Scholor - Essayas A, Legesse M, Tila M, Sintayhu A, Abreham E, Dendir G. (2024). Effects of 4 mg and 8 mg Dexamethasone Added to Intrathecal Bupivacaine on Perioperative Analgesia Among Adult Orthopedic Patients at Sodo Christian Hospital: A Prospective Cohort Study. Pain Research and Management, 2024(1):8872988.
Publisher | Google Scholor - Fayyaz, M. A., Khan, A. A., & Ali, R. L. (2015). Comparison between effect of bupivacaine and bupivacaine with dexamethasone on duration of analgesia in spinal anesthesia for elective caesarean section. PJMHS, 9:979-982.
Publisher | Google Scholor - Bani-Hashem N, Hassan-Nasab B, Pour EA, Maleh PA, Nabavi A, Jabbari A. (2011). Addition of intrathecal Dexamethasone to Bupivacaine for spinal anesthesia in orthopedic surgery. Saudi J Anaesth. 5(4):382-386.
Publisher | Google Scholor - Alarasan, A. K., Agrawal, J., Choudhary, B., Melhotra, A., Uike, S., & Mukherji, A. (2016). Effect of dexamethasone in low volume supraclavicular brachial plexus block: A double-blinded randomized clinical study. Journal of Anaesthesiology Clinical Pharmacology, 32(2):234-239.
Publisher | Google Scholor - Esmat, I. M., Elsayed, A. M., El-Hariri, H. M., & Ashoor, T. M. (2022). A randomized controlled trial for prevention of postspinal anesthesia shivering in gynecological surgeries: Mirtazapine vs. dexamethasone. Anesthesiology Research and Practice, 5061803.
Publisher | Google Scholor























