

Case Report
Bleeding Lungs in the Tropics: A Case of Leptospirosis-Associated Diffuse Alveolar Hemorrhage
- M. Gines-Rosario MD, MHA *
- B. Lopez MD
- V. De La Rosa, MD
- M.C. Betancourt, MD
- M.C. Perez-Mitchell, MD
- R. Fernandez, MD
Department of Internal Medicine, Department of Pulmonary and Critical Care Medicine, San Juan City Hospital, San Juan, Puerto Rico, United States.
*Corresponding Author: M. Gines-Rosario MD, MHA, Department of Internal Medicine, Department of Pulmonary and Critical Care Medicine, San Juan City Hospital, San Juan, Puerto Rico, United States.
Citation: Gines-Rosario M., López B., Rosa V. De La, Betancourt M.C., Pérez-Mitchell M.C., et al. (2025). Bleeding Lungs in the Tropics: A Case of Leptospirosis-Associated Diffuse Alveolar Hemorrhage, Clinical Case Reports and Studies, BioRes Scientia Publishers. 10(3):1-3. DOI: 10.59657/2837-2565.brs.25.261
Copyright: © 2025 Mariela Gines Rosario, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: June 12, 2025 | Accepted: June 26, 2025 | Published: July 03, 2025
Abstract
Leptospirosis is a serious infection caused by spirochete bacteria, typically spread through contact with contaminated water, soil, or animals which poses significant public health challenges, particularly in tropical and subtropical regions. Clinical presentation can range from non-specific flu-like symptoms to more severe forms that may lead to Weil’s disease, characterized by jaundice, renal failure, and bleeding complications. One such complication is diffuse alveolar hemorrhage (DAH), which can cause acute respiratory failure requiring intensive care support. This condition is characterized by the accumulation of blood in the alveolar spaces of the lungs, leading to respiratory distress and hypoxemia. Understanding the pathophysiological links between leptospirosis and DAH is crucial for timely diagnosis and management. This case report aims to highlight the clinical significance of leptospirosis and its potential to lead to diffuse alveolar hemorrhage, emphasizing the need for heightened awareness and prompt intervention in affected individuals. Further research into the mechanisms underlying this association may enhance treatment strategies and improve patient outcomes.
Keywords: leptospira; lung complications; alveolar hemorrhage; febrile illness
Introduction
Leptospirosis is a globally prevalent zoonotic infection caused by pathogenic Leptospira species, typically transmitted through contact with contaminated water, soil, or animal urine. The clinical spectrum is broad, ranging from a mild, self-limited febrile illness to severe, life-threatening disease characterized by multiorgan dysfunction. Weil's disease — a severe form-classically includes jaundice, renal failure, and hemorrhagic manifestations. One of the most ominous pulmonary complications is diffuse alveolar hemorrhage (DAH), a rare but potentially fatal condition resulting from disruption of the alveolar-capillary membrane [1]. DAH in leptospirosis is uncommon, yet its presence often portends a fulminant course. We describe a case of leptospirosis-associated DAH in a previously healthy adult, emphasizing the critical care management challenges and therapeutic considerations.
Case Presentation
A 44-year-old male with a history of chronic alcohol use presented with a 7-day history of fever, myalgias, weakness, and progressive abdominal distention. On examination, he appeared icteric, with scleral icterus, left conjunctival suffusion, and ascites. Laboratory workup revealed severe hyponatremia (Na: 102 mEq/L), leukocytosis (WBC: 15.6 x10%L), and marked hyperbilirubinemia (total bilirubin: 16.5 mg/dL). A chest radiograph showed a patchy pneumonic process. Given his epidemiologic risk and clinical findings, leptospirosis was suspected. Empiric therapy with intravenous ceftriaxone and doxycycline was initiated, and Leptospira IgM testing was sent. Despite early antimicrobial treatment, the patient's condition deteriorated, requiring ICU transfer for septic shock management with vasopressors. Broad-spectrum antibiotics (vancomycin and piperacillin-tazobactam) were initiated. He subsequently developed worsening hypoxemic respiratory failure, necessitating mechanical ventilation. High-resolution CT of the chest demonstrated bilateral diffuse progression of multifocal ground-glass opacities, in the presence of worsening hemoptysis which is consistent with DAH (Figures 2 A / B). A bronchoalveolar lavage was subsequently performed, which confirmed the diagnosis. Ventilatory management included high PEEP, increased FiO2, and lung-protective tidal volumes. Adjunctive corticosteroid therapy was initiated. However, persistent bloody endotracheal secretions indicated ongoing alveolar bleeding, complicating ventilatory strategies. Prone positioning was employed as a salvage maneuver, but the patient's course was further complicated by multiorgan failure.
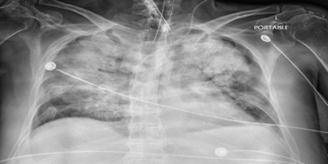
Figure 1A: Chest X-ray revealing bilateral diffuse, non-homogeneous fluffy opacities, along with lung infiltrates and haziness indicative of edema, hemorrhage, or pneumonia. Additionally, there is a small pleural effusion on the left side.
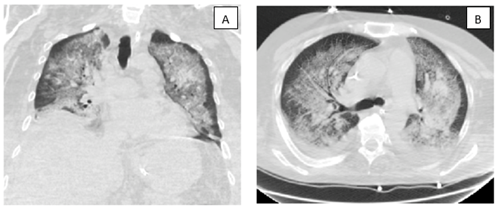
Figure 2 A / B: Chest CT scan demonstrating marked progression of multifocal confluent opacities, as can be seen in the setting of diffuse pulmonary hemorrhage.
Discussion
This case underscores the rare but potentially catastrophic pulmonary manifestation of leptospirosis: diffuse alveolar hemorrhage (DAH). Although pulmonary involvement in leptospirosis is increasingly recognized, DAH remains an infrequent but severe complication associated with high mortality [1]. The underlying pathophysiology is believed to involve immune-mediated capillary injury, where leptospiral antigens trigger a cascade of inflammatory responses resulting in disruption of the alveolar-capillary barrier. This leads to extravasation of red blood cells into the alveolar spaces, culminating in hemorrhagic pulmonary infiltrates and hypoxemic respiratory failure. Diagnosis of DAH in the context of leptospirosis can be particularly challenging, as early clinical features are often nonspecific and mimic other infectious or inflammatory pulmonary syndromes [2,3]. Hemoptysis may be absent or minimal, further complicating timely recognition. Radiologic findings—such as bilateral ground-glass opacities or consolidations—are nonspecific and must be interpreted in conjunction with clinical suspicion and bronchoalveolar lavage findings demonstrating progressively hemorrhagic aliquots. Prompt recognition is critical, as rapid deterioration and progression to acute respiratory distress syndrome (ARDS) are common [1]. Mortality rates in leptospiral DAH can exceed 50%, particularly when diagnosis and escalation of care are delayed. Management is predominantly supportive, emphasizing lung-protective mechanical ventilation strategies to minimize ventilator-induced lung injury. Adjunctive therapies such as high-dose corticosteroids are frequently administered based on presumed immunopathogenesis, though robust evidence from controlled trials remains lacking [4]. In severe or refractory cases, additional interventions—including plasmapheresis, bronchial artery embolization, or extracorporeal membrane oxygenation (ECMO)—may be necessary to stabilize oxygenation and provide a bridge to recovery while hemorrhage control is achieved [6]. This case highlights the importance of maintaining a high index of suspicion for leptospiral DAH in endemic areas or in patients with appropriate exposure history, particularly when presenting with unexplained respiratory failure. Further research is urgently needed to better define optimal diagnostic and therapeutic approaches, as current management is largely extrapolated from case series and expert opinion.
Conclusion
Leptospirosis-associated DAH presents a formidable diagnostic and therapeutic challenge. Early clinical suspicion, timely antimicrobial therapy, and aggressive critical care management are essential to improving outcomes. This case highlights the need for heightened awareness of DAH as a potential complication in patients presenting with severe leptospirosis, particularly in endemic regions or those with high environmental exposure risk.
References
- Barnacle, J., Gurney, S., Ledot, S. et al. (2020). Leptospirosis as an important differential of pulmonary hemorrhage on the intensive care unit: a case managed with VV-ECMO. j intensive care 8:31.
Publisher | Google Scholor - Dong, W. H., & Chen, Z. (2021). Leptospirosis with pulmonary hemorrhage and multiple organ failure: a case report and literature review. The Journal of international medical research, 49(5):3000605211019665.
Publisher | Google Scholor - Jones, F. K., Medina, A. G., Ryff, K. R., et al. (2024). Leptospirosis Outbreak in Aftermath of Hurricane Fiona - Puerto Rico, 2022. MMWR. Morbidity and mortality weekly report, 73(35):763–768.
Publisher | Google Scholor - Nicodemo, A. C., & Duarte-Neto, A. N. (2021). Pathogenesis of Pulmonary Hemorrhagic Syndrome in Human Leptospirosis. The American journal of tropical medicine and hygiene, 104(6):1970–1972.
Publisher | Google Scholor - Zhang, Y., Hongyi, T., Xiaoli, S., et al. (2016). A Case Report of Leptospirosis with Extensive Alveolar Hemorrhage. CHEST, Volume 149(4):A72.
Publisher | Google Scholor























