

Research Article
Association Between Age of Patient and Grade of Breast Cancer
- Shumaila Nawaz Khan *
- Ghulam Haider
- Kaneez Zainab Rabail
- Saima Zahoor
- Abdul rehman
- Aakash Ramchand
- Munazza Anwer
- Mehwish Jabeen
Innah post graduate medical center (JPMC), Pakistan.
*Corresponding Author: Shumaila Nawaz Khan, Innah post graduate medical center (JPMC), Pakistan.
Citation: Shumaila N. Khan, Haider G, Kaneez Z. Rabail, Zahoor S, Rehman A, et al. (2025). Association Between Age of Patient and Grade of Breast Cancer. Journal of BioMed Research and Reports, BioRes Scientia Publishers. 7(1):1-8. DOI: 10.59657/2837-4681.brs.25.128
Copyright: © 2025 Shumaila Nawaz Khan, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: January 11, 2025 | Accepted: January 25, 2025 | Published: February 01, 2025
Abstract
Objectives: The objective of this study was to investigate the association between age of patients and histologic grade of breast cancer, to better understand how age affects tumor grade.
Methodology: This cross-sectional study was conducted at a single center and included women diagnosed with breast cancer between the ages of 18 and 80 years. The patients were categorized into different age groups, and tumor characteristics, including histological grade, tumor size, and lymph node involvement, were assessed. Statistical analysis was performed to identify significant associations between age and these characteristics, especially grade using Chi-square and Fisher’s exact tests.
Results: No significant relationship was observed between age and histological grade (p=0.237). However, significant associations were found between age and axillary lymph node involvement (p=0.01) as well as TNM staging (p=0.03), with younger and older patients showing more advanced disease.
Conclusion: This study shows there is no significant association between age of patients and histologic grade of breast cancer. Further research with larger, multi-center studies is needed to validate these findings.
Keywords: breast cancer; tumor characteristics; lymph node involvement; tnm staging; prognosis; age-specific management
Introduction
Breast Cancer is the most common cancer in women in most parts of the world, with a marked geographic variation in incidence in different countries. The incidence is highest in Northern Europe and North America, intermediate in the Mediterranean and South America, and lowest in Asia and Africa [1]. Breast cancer comprises 18% of all female cancers.2 It is the second leading cause of death from cancer among women [3], affecting up to one in 11 women during life [4]. According to the American Cancer Society report, breast cancer is diagnosed in about 1.3 million women annually worldwide, and around 465,000 die from the disease [5]. Of every 1000 women of 50 years of age, two will have recently had breast cancer diagnosed and about 15 will have had a diagnosis made before the age of 50 years, giving the breast cancer a prevalence of 2% [2]. According to National Cancer Registries in different Asian countries, the crude incidence rate of breast cancer varied from 21.3 per 100,000 populations in Jordan, 21.4 in Iran, 24.1 in Turkey, 34.86 in Malaysia, and 48 in Japan [1]. It accounts for 19-34% of all cancers in India [6] and 19.1% in Saudi Arabia [2].
Karachi Cancer Registry, the only population-based cancer registry in Pakistan, reports breast cancer as the most common cancer (34.6% of cancer cases) among females. The age-standardized incidence rate (to the world population) was 69.1 per 100,000 averaged over the years 1998-2002, the highest recorded rate of breast cancer in Asia. Similarly in Lahore, another major city of Pakistan, breast cancer is the most common female cancer [7]. International Association of Cancer Research, based in France, projected that there would be 250,000 cases of breast cancer in India by 2015 a 3% increase per year currently, and undoubtedly breast cancer will become an epidemic in India and Pakistan in another ten years [8]. The incidence of breast cancer increases up to the age of 80 years, between the ages of 80-85 years, and then declines [2]. Breast cancer occurs in a younger age group of Asian women, 40-49 years old compared to the West, where the peak prevalence is seen between 50 – 59 years [1].
Many developed countries offer the National Breast Cancer Screening Programme, whereas in developing countries screening is assessed by individuals who can afford it [9]. Recommendations for countries with limited resources and WHO emphasized that the national breast cancer control program should encourage early diagnosis of breast cancer, especially for women aged 40-69 years [10]. Third-world breast cancer is characterized by late presentation, advanced stage of disease with worse biological behaviors, and occurrence relatively at a younger age [11]. In developing countries, patients with breast cancer present for the first time in an advanced stage (stage 2 to 3) [12]. Multiple factors like psychosocial and cultural beliefs, non-availability of treatment facilities, illiteracy, poverty, lack of awareness about breast cancer, and fear of surgery are believed to be responsible for this late presentation [11]. Particularly in Islamic countries, generally, women abstain from touching their breast, do not go for CBE (clinical breast examination) and feel embarrassed of undergoing mammography [13]. Trend in a change in age pattern has been noted in various studies. However, the association between age and grade of breast cancer has not been well studied.
Pakistan is a developing country with limited resources. Therefore, early detection of breast cancer can secure women against premature mortality, physical defects as well as psychological distress. Screening awareness is strongly recommended because the incidence of breast cancer is rising, and the mortality rate is high due to delayed diagnosis and insufficient public awareness. Knowing the grade of cancer and its association with different age groups will be helpful in the management of breast cancer in various age groups. Background lacking, theoretically, young patients have high-grade tumors as compared to older age patients according to several studies and reports. The present study aimed to determine the association between the age of the patient and the grade of breast cancer.
Methods and Materials
The study was a cross-sectional survey conducted in the Department of Medical Oncology at Jinnah Postgraduate Medical Center (JPMC) Hospital in Karachi. The study spanned six months following the Institutional Review Board (IRB) approval. The sample size was calculated using the W.H.O. sample size calculator, with a frequency for grade I breast cancer among women aged ≤40 years and >40 years taken as 2.7% and 10.2%, respectively. The power of the test was set at 80%, with a level of significance (α) of 5%. This yielded an estimated sample size of 66 participants in each group, leading to a total of 132 participants. Non-probability consecutive sampling was employed for patient selection. Participants were selected based on the following inclusion criteria: women aged 18 to 80 years who were diagnosed with breast cancer according to operational definitions, had a cancer duration of 24 weeks, and represented all stages of breast cancer. Exclusion criteria included patients unwilling to participate, patients with a history of breast trauma, and pregnant or lactating women.
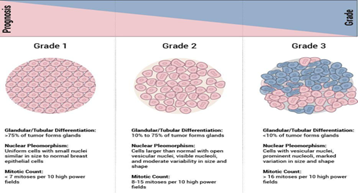
Before enrollment, the study was explained in detail to each eligible participant, and written informed consent was obtained. Baseline demographic and clinical details, including age, residence, education, marital status, height (measured using a wall-mounted scale in centimeters), weight (measured using a digital weighing machine with light clothing), and BMI (calculated as Weight in Kg / Height in m²), were recorded in a predesigned proforma. Participants aged ≤40 years were assigned to Group A, while those aged >40 years were categorized in Group B. Each participant underwent screening for breast carcinoma, which included immunohistochemical staining and histological grading based on a histopathology report. The histological grading of breast cancer was performed using the Scarff-Bloom-Richardson grading system.
To minimize bias and confounders, strict adherence to the exclusion criteria was maintained, ensuring that only relevant data were included in the analysis. Data were entered and analyzed using SPSS version 24.0. Descriptive statistics, including the mean ± SD or median (IQR), were calculated for continuous variables such as age, weight, height, BMI, and family monthly income. Categorical variables like residential status, marital status, educational level, diabetes mellitus, hypertension, family history of breast cancer, and breast cancer grades were summarized using frequencies and percentages. The association between breast cancer grades and age was analyzed using the Chi-square test or Fisher's exact test, as appropriate. To control for confounding variables (age groups, BMI, residential status, marital status, educational level, diabetes, hypertension, family history of breast cancer, and family income), stratification was applied. Post-stratification, Chi-square or Fisher's exact tests were conducted, with a p-value ≤ 0.05. Bar graphs and pie charts were used to present the graphical representation of the data, ensuring a clear visualization of the results.
Results
The mean age at presentation for the participants was 47.3 years with a standard deviation of 12.63. The mean age at menarche was 12.72 years with a standard deviation of 1.64 (Table 1).
Table 1: Age at presentation and menarche
| Variables | Mean (SD) |
| Age at presentation | 47.3 (12.63) |
| Age at menarche | 12.72 (1.64) |
The age distribution of the participants was as follows: <30>70 years, 2 (1.7%). Marital status showed that 102 (85%) were married and 18 (15%) were unmarried. Regarding parity, 92 (76.7%) had children and 28 (23.3%) did not. Ethnic distribution included Sindhi, 32 (26.7%); Urdu, 54 (45%); Punjabi, 22 (18.3%); Pashto, 5 (4.2%); Balochi, 3 (2.5%); and Other, 4 (3.3%). Family history of cancer was reported in 49 (40.8%) participants, while 71 (59.2%) had no family history. A family history of breast cancer was present in 42 (35%) participants, and absent in 78 (65%). Menopausal status was almost evenly split, with 63 (52.5%) being premenopausal and 57 (47.5%) postmenopausal. Body Mass Index (BMI) showed the following distribution: <18>30, 5 (4.2%). Lastly, 92 (76.7%) participants had a history of lactation, while 28 (23.3%) did not.
Table 2: Sociodemographic variables of participants
| Variables | N | % |
| Age Group | ||
| <30> | 9 | 7.5 |
| 30-50 years | 75 | 62.5 |
| 51-70 | 34 | 28.3 |
| >70 years | 2 | 1.7 |
| Marital status | ||
| Married | 102 | 85 |
| Unmarried | 18 | 15 |
| Parity | ||
| Yes | 92 | 76.7 |
| No | 28 | 23.3 |
| Ethnicity | ||
| Sindhi | 32 | 26.7 |
| Urdu | 54 | 45 |
| Punjabi | 22 | 18.3 |
| Pashto | 5 | 4.2 |
| Balochi | 3 | 2.5 |
| Other | 4 | 3.3 |
| Family history of cancer | ||
| Yes | 49 | 40.8 |
| No | 71 | 59.2 |
| Family history of breast cancer | ||
| Yes | 42 | 35 |
| No | 78 | 65 |
| Menopausal Status | ||
| Premenopausal | 63 | 52.5 |
| Postmenopausal | 57 | 47.5 |
| Body Mass Index | ||
| <18> | 4 | 3.3 |
| >18-23 | 4 | 3.3 |
| 23-25 | 62 | 51.7 |
| 25-30 | 45 | 37.5 |
| >30 | 5 | 4.2 |
| Lactation | ||
| Yes | 92 | 76.7 |
| No | 28 | 23.3 |
The clinical characteristics of the patients are as follows: the cancer was located on the left side in 43 (35.8%), on the right side in 71 (59.2%), and was bilateral in 6 (5%) patients. The histological type was infiltrating ductal carcinoma in 101 (84.2%), lobular carcinoma in 17 (14.2%), and other types in 2 (1.7%). Histological grading showed that 6 (5%) patients had grade I, 78 (65%) had grade II, and 36 (30%) had grade III cancer. The Ki67 index was <20>21% in 88 (73.3%) patients. Tumor size was <2>5 cm in 55 (45.8%), with 1 (0.8%) having an unknown size. Multifocal or multicentric tumors were present in 29 (24.2%) patients, while 91 (75.8%) did not have multifocal/multicentric tumors. Axillary lymph node involvement was present in 90 (75%) patients and absent in 30 (25%). Regarding TNM staging, 7 (5.8%) patients were in stage I, 46 (38.3%) in stage II, 54 (45%) in stage III, and 13 (10.8%) in stage IV. Nuclear grading showed 9 (7.5%) in grade I, 75 (62.5%) in grade II, and 36 (30%) in grade III. HER2 status was positive in 45 (37.5%), negative in 67 (55.8%), borderline in 5 (4.2%), and unknown in 3 (2.5%). Estrogen receptor status was positive in 75 (62.5%) patients and negative in 45 (37.5%). Progesterone receptor status was positive in 57 (47.5%) and negative in 63 (52.5%) (Table 3).
Table 3: Clinical characteristics of patients
| Characteristics | N | % |
| Side | ||
| Left | 43 | 35.8 |
| Right | 71 | 59.2 |
| Bilateral | 6 | 5 |
| Histological type | ||
| Infiltrating duct | 101 | 84.2 |
| Lobular | 17 | 14.2 |
| Others | 2 | 1.7 |
| Histological grade | ||
| I | 6 | 5 |
| II | 78 | 65 |
| III | 36 | 30 |
| Ki67 | ||
| <20> | 32 | 26.7 |
| >21% | 88 | 73.3 |
| Tumor size | ||
| <2> | 6 | 5 |
| 2-5 cm | 58 | 48.3 |
| >5 cm | 55 | 45.8 |
| 5 | 1 | 0.8 |
| Multifocal /Multicentric | ||
| Yes | 29 | 24.2 |
| No | 91 | 75.8 |
| Axillary lymphnode | ||
| Yes | 90 | 75 |
| No | 30 | 25 |
| TNM Stage | ||
| I | 7 | 5.8 |
| II | 46 | 38.3 |
| III | 54 | 45 |
| IV | 13 | 10.8 |
| Nuclear stage | ||
| I | 9 | 7.5 |
| II | 75 | 62.5 |
| III | 36 | 30 |
| HER2 status | ||
| Positive | 45 | 37.5 |
| Negative | 67 | 55.8 |
| Borderline | 5 | 4.2 |
| Unknown | 3 | 2.5 |
| Estrogen Receptor | ||
| Positive | 75 | 62.5 |
| Negative | 45 | 37.5 |
| Progesterone Receptor | ||
| Positive | 57 | 47.5 |
| Negative | 63 | 52.5 |
For histological grade, grade I was found only in the 30-50 age group, accounting for 6 (100%) of the cases (p=0.237). Grade II was observed in 4 (5.1%) patients under 30 years, 50 (64.1%) patients aged 30-50 years, 22 (28.2%) patients aged 51-70 years, and 2 (2.6%) patients over 70 years. Grade III was found in 5 (13.9%) patients under 30 years, 19 (52.8%) in the 30-50 age group, 12 (33.3%) aged 51-70 years. However, histological grade was not significantly associated with age of patient (p=0.237). Significant associations (p less than 0.05) were found for axillary lymph node involvement (p=0.01) and TNM stage (p=0.03). This suggests that age groups were significantly associated with the likelihood of axillary lymph node involvement and TNM staging, indicating a potential impact of age on these specific clinical characteristics. For axillary lymph node involvement, 8 (8.9%) under 30 years, 52 (57.8%) aged 30-50, 30 (33.3%) aged 51-70 had involvement, while 1 (3.3%) under 30 years, 23 (76.7%) aged 30-50, 4 (13.3%) aged 51-70, and 2 (6.7%) over 70 years had no involvement (p=0.01). For TNM stage, stage I occurred in 5 (71.4%) aged 30-50, 1 (14.3%) aged 51-70, and 1 (14.3%) over 70 years (p=0.03). Stage II was found in 1 (2.2%) under 30, 33 (71.7%) aged 30-50, 11 (23.9%) aged 51-70, and 1 (2.2%) over 70 years. Stage III occurred in 5 (9.3%) under 30, 32 (59.3%) aged 30-50, and 17 (31.5%) aged 51-70. Stage IV occurred in 3 (23.1%) under 30, 5 (38.5%) aged 30-50, and 5 (38.5%) aged 51-70.
Table 4: Association of Age groups with tumor characteristics
| Age Group | Total | p-value | ||||
| Histological grade | <30> | 30-50 years | 51-70 | >70 years | ||
| Grade I | - | 6 (100%) | - | - | 6 (100%) | 0.237 |
| Grade II | 4 (5.10%) | 50 (64.10%) | 22 (28.20%) | 2 (2.60%) | 78 (100%) | |
| Grade III | 5 (13.9%) | 19 (52.80%) | 12 (33.30%) | - | 36 (100%) | |
| Histological Type | ||||||
| Infiltrating duct | 9 (8.9%) | 62 (61.4%) | 29 (28.7%) | 1 (1%) | 101 (100%) | 0.559 |
| Lobular | - | 11 (64.7%) | 5 (29.4%) | 1 (5.9%) | 17 (100%) | |
| Others | - | 2 (100%) | - | - | 2 (100%) | |
| Tumor size | ||||||
| <2> | - | 5 (83.3%) | 1 (16.7%) | - | 6 (100%) | 0.857 |
| 2-5 cm | 3 (5.2%) | 37 (63.8%) | 17 (29.3%) | 1 (1.7%) | 58 (100%) | |
| >5 cm | 6 (10.9%) | 33 (60%) | 16 (28.6%) | 1 (1.8%) | 56 (100%) | |
| Multifocal/Multicentric lesion | ||||||
| Yes | 1 (3.4%) | 19 (65.5%) | 8 (27.6%) | 1 (3.4%) | 29 (100%) | 0.653 |
| No | 8 (8.8%) | 56 (61.5%) | 26 (28.6%) | 1 (1.1%) | 91 (100%) | |
| Axillary lymph node | ||||||
| Yes | 8 (8.9%) | 52 (57.8%) | 30 (33.3%) | - | 90 (100%) | 0.01 |
| No | 1 (3.3%) | 23 (76.7%) | 4 (13.3%) | 2 (6.7%) | 30 (100%) | |
| TNM Stage | ||||||
| I | - | 5 (71.4%) | 1 (14.3%) | 1 (14.3%) | 7 (100%) | 0.03 |
| II | 1 (2.2%) | 33 (71.7%) | 11 (23.9%) | 1 (2.2%) | 46 (100%) | |
| III | 5 (9.3%) | 32 (59.3%) | 17 (31.5%) | - | 54 (100%) | |
| IV | 3 (23.1%) | 5 (38.5%) | 5 (38.5%) | - | 13 (100%) | |
| Nuclear Stage | ||||||
| I | - | 6 (66.7%) | 3 (33.3%) | - | 9 (100%) | 0.456 |
| II | 4 (5.3%) | 50 (66.7%) | 19 (25.3%) | 2 (2.7%) | 75 (100%) | |
| III | 5 (13.9%) | 19 (52.8%) | 12 (33.3%) | - | 36 (100%) | |
| HER2 status | ||||||
| Positive | 3 (6.7%) | 31 (68.9%) | 9 (20%) | 2 (4.4%) | 45 (100%) | 0.356 |
| Negative | 6 (9%) | 39 (58.2%) | 22 (32.8%) | - | 67 (100%) | |
| Borderline | - | 2 (40%) | 3 (60%) | - | 5 (100%) | |
| Unknown | - | 3 (100%) | - | - | 3 (100%) | |
Discussion
The study found significant associations between age and specific tumor characteristics, particularly axillary lymph node involvement and TNM staging, suggesting that younger patients may present with more advanced disease. Understanding the relationship between age and breast cancer features is crucial for guiding personalized treatment strategies and improving prognosis, especially in resource-limited settings where early detection can be challenging.
The findings from this study align with those of several previous investigations regarding age-related breast cancer characteristics. Fernandes et al. (2023) similarly found that younger women tend to present with more aggressive disease, showing a higher prevalence of advanced TNM stages and lymph node involvement(fernandes). Additionally, Xie et al. (2023) reported a U-shaped relationship between age and breast cancer outcomes, with both younger and older women exhibiting worse survival rates than middle-aged women, further supporting the age-related variation in breast cancer behavior(xie). Rosenberg et al. (2005) also confirmed that tumor size and grade significantly impact survival across age groups, particularly highlighting the negative effect of larger tumors in younger women(rossenberg). The study’s finding of significant associations between age, axillary lymph node involvement, and TNM staging is particularly noteworthy. Tadros et al. (2020) demonstrated that younger women undergoing surgery for breast cancer often experience more frequent lymph node involvement compared to older women(tadros). This could be attributed to more aggressive tumor biology, as highlighted by Amalie et al. (2024), who emphasized that younger patients are more likely to have HER2-positive and triple-negative subtypes, which are linked to higher proliferation rates and poorer prognosis(amalie). Furthermore, Lodi et al. (2024) found that while elderly women tend to present with more advanced local stages, younger women are more likely to develop lymph node metastasis at earlier stages, indicating distinct biological behavior based on age(lodi). Clinically, these findings suggest that younger and older women may benefit from age-specific screening and treatment strategies, particularly regarding early detection and the management of lymph node metastasis.
The lack of significant associations between age and histological grade, histological type, and tumor size in this study could be influenced by the sample size or the heterogeneity of breast cancer. While Chen et al. (2016) found that younger women are more likely to present with larger tumors and more aggressive histological types, this is not consistently observed across all age groups(chen). Additionally, the study by Di Saverio et al. (2007) suggested that despite some variation in tumor grade across age groups, other factors, such as hormone receptor status and Ki67 expression, may play a more dominant role in determining tumor behavior(s10549-007-9809-z). Future studies with larger cohorts are needed to explore these variables further and refine treatment personalization based on age. This study has several limitations, including its relatively small sample size and single-center design, which may limit the generalizability of the findings. Additionally, potential confounding factors such as variations in treatment protocols and genetic predispositions were not controlled for. These limitations suggest that the results should be interpreted cautiously, and broader studies are needed to confirm the findings. Future research should focus on larger, multi-center studies to validate these findings and explore the role of age in breast cancer prognosis across diverse populations. Age-specific management strategies should be developed to optimize treatment outcomes, particularly in younger and older women. Incorporating these insights into clinical practice is crucial, especially in resource-limited settings, where tailored screening and early detection programs could significantly improve survival rates.
Conclusion
This study highlights the significant association between age and breast cancer characteristics, particularly axillary lymph node involvement and TNM staging, indicating that younger and older patients may present with more aggressive forms of the disease. Although age was not significantly associated with other tumor characteristics such as histological grade, type, or tumor size, the findings underscore the need for age-specific management strategies in breast cancer care. Tailored screening and treatment approaches, especially for younger and older populations, could improve early detection and outcomes. Integrating age-specific insights into clinical practice is essential for improving the prognosis of breast cancer patients, particularly in resource-limited settings where early detection and personalized care can significantly impact survival and quality of life.
Performa
Annexure I: Scarff-Bloom-Richardson grading system
References
- Abusaleem, O., & Hassan, M. A. (2007). Breast self-examination among female nurses. Rawal Medical Journal, 32(1):30-32.
Publisher | Google Scholor - Ahmed, F., Mahmud, S., Hatcher, J., & Khan, S. M. (2006). Breast cancer risk factor knowledge among nurses in teaching hospitals of Karachi, Pakistan: A cross-sectional study. BMC Nursing, 5:6.
Publisher | Google Scholor - Bala, D. V., & Gameti, H. (2011). An educational intervention study of breast self-examination in 250 women beneficiaries of urban health centers of west zone of Ahmedabad. Healthline, 2(2):46-48.
Publisher | Google Scholor - Chen, H., Zhou, M., Tian, W., Meng, K., & He, H. (2016). Effect of age on breast cancer patient prognoses: A population-based study using the SEER 18 database. PLoS ONE, 11(10):e0165409.
Publisher | Google Scholor - Di Saverio, S., Gutierrez, J., & Avisar, E. (2007). A retrospective review with long-term follow-up of 11,400 cases of pure mucinous breast carcinoma. Breast Cancer Research and Treatment, 111(3):541-547.
Publisher | Google Scholor - Fernandes, J. O., Cardoso-Filho, C., Kraft, M. B., Detoni, A. S., Duarte, B. N., Shinzato, J. Y., & Vale, D. B. (2023). Differences in breast cancer survival and stage by age in off-target screening groups: A population-based retrospective study. American Journal of Obstetrics and Gynecology Global Reports, 100208:1-10.
Publisher | Google Scholor - Harirchi, I., Mousavi, S. M., Mohagheghi, M. A., Jarrahi, A. M., Ebrahimi, M., & Montazeri, A. (2009). Do knowledge, attitudes, and practices of Iranian healthcare providers meet WHO recommendations on early detection for breast cancer? Asian Pacific Journal of Cancer Prevention, 10:849-851.
Publisher | Google Scholor - Jaradeen, N. K. (2010). Breast cancer risk factors and breast self-examination practice among Jordanian women. Bahrain Medical Bulletin, 32(1):1-7.
Publisher | Google Scholor - Lodhi, F. B., Ahmad, B., Shah, S. I. H., Naeem, M., Dab, R. H., & Ali, N. (2010). Determinants of delayed presentation in breast cancer. APMC, 4(1):9-16.
Publisher | Google Scholor - Lodi, M., Bousquet, N., Valverde, P., De la Ferrière, M., Neuberger, et al. (2024). Breast cancer characteristics in elderly women: A comprehensive cohort study of 7,965 patients. Innovative Practice in Breast Health, 1:100001.
Publisher | Google Scholor - Obaikol, R., Galukande, M., & Fualal, J. (2010). Knowledge and practice of breast self-examination among female students in a Sub-Saharan African university. East and Central African Journal of Surgery, 15(1):22-27.
Publisher | Google Scholor - Ozkan, A., Malak, A. T., Gurkan, A., & Turgay, A. S. (2010). Do Turkish nursing and midwifery students teach breast self-examination to their relatives? Asian Pacific Journal of Cancer Prevention, 11:1569-1573.
Publisher | Google Scholor - Parajuli, P., & Mandal, G. N. (2010). Knowledge about breast cancer and breast self-examination practices among medical, dental, and B.Sc. nursing students of BPKIHS. Health Renaissance, 8(3):166-168.
Publisher | Google Scholor - Parsa, P., Kandiah, M., Rahman, H. A., & Zulkefli, N. A. (2006). Barriers for breast cancer screening among Asian women. Asian Pacific Journal of Cancer Prevention, 7:509-514.
Publisher | Google Scholor - Parvani, Z. (2011). Breast self-examination; Breast awareness and practices: A systematic review. Professional Medical Journal, 18(2):336-339.
Publisher | Google Scholor - Rosenberg, J., Chia, Y. L., & Plevritis, S. (2005). The effect of age, race, tumor size, tumor grade, and disease stage on invasive ductal breast cancer survival in the U.S. SEER database. Breast Cancer Research and Treatment, 89(1):47-54.
Publisher | Google Scholor - Svanøe, A. A., Humlevik, R. O. C., Knutsvik, G., Sæle, A. K. M., et al. (2024). Age-related phenotypes in breast cancer: A population-based study. International Journal of Cancer, 154(2):2014-2024.
Publisher | Google Scholor - Tadros, A. B., Moo, T. A., Stempel, M., Zabor, E. C., Khan, A. J., & Morrow, M. (2020). Axillary management for young women with breast cancer varies between patients electing breast-conservation therapy or mastectomy. Breast Cancer Research and Treatment, 180(1):197-205.
Publisher | Google Scholor - Xie, Y., Deng, Y., Wei, S., Huang, Z., Li, L., et al. (2023). Age has a U-shaped relationship with breast cancer outcomes in women: A cohort study. Frontiers in Oncology, 13:1265304.
Publisher | Google Scholor - Yadav, P., & Jaroli, D. P. (2010). Breast cancer: Awareness and risk factors in college-going younger age group women in Rajasthan. Asian Pacific Journal of Cancer Prevention, 11:319-322.
Publisher | Google Scholor























