

Research Article
Anxiety Level of Caregivers of Children with Common Congenital Lower Limb Deformities
1Final Year Student of BSc (Hons) Orthotics & Prosthetics, Rawalpindi Medical University, Rawalpindi, Punjab, Pakistan.
2Course Supervisor & Senior Registrar Orthopedics, Benazir Bhutto Hospital, Rawalpindi, Pakistan.
3Course Co-coordinator & Clinical Supervisor, Benazir Bhutto Hospital, Rawalpindi, Pakistan.
4Assistant Professor Community Medicine, Rawalpindi Medical University, Rawalpindi, Punjab, Pakistan.
*Corresponding Author: Rizwana Shahid, Assistant Professor Community Medicine, Rawalpindi Medical University, Rawalpindi, Punjab, Pakistan.
Citation: Altaf B, Khan AN, Javaid A, Shahid R. (2025). Anxiety Level of Caregivers of Children with Common Congenital Lower Limb Deformities, International Journal of Biomedical and Clinical Research, BioRes Scientia Publishers. 4(5):1-5. DOI: 10.59657/2997-6103.brs.25.093
Copyright: © 2025 Rizwana Shahid, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: September 15, 2025 | Accepted: October 16, 2025 | Published: October 23, 2025
Abstract
Background: Congenital lower limb deformities prevail at birth either due to aplasia or hypoplasia of bone during fetal development. These deformities can occur either transversely or longitudinally and can be complete or incomplete. One or more bones can be involved. Such deformities may likely to diminish the joy of childbirth with emotional disturbance of their guardians. The present study is therefore meant to measure the anxiety level of caregivers of the children diagnosed with congenital lower limb deformities.
Subjects & Methods: A cross-sectional descriptive study was done among 100 caregivers of the children with established lower limb deformities who were enrolled in the study through purposive sampling. The responses were gathered from caregivers by using Standardized Hamilton Anxiety Rating Scale (HAM-A). Data was entered and analyzed by using SPSS version 25 and MS Excel 2019. Descriptive statistics were applied.
Results: Responses of the 56 male and 44 female caregivers pertaining to their anxiety level due to children with congenital lower limb deformities were collected. Mean age of the respondents were 21.7 ± 9.2 years. Developmental Dysplasia of Hip (DDH) was maximally (21%) reported followed by Leg Length Discrepancy (LLD) (19%) and Pes Planus (17%). About 67 caregivers had mild to moderate anxiety with score in the range of 18-24 while 20 caregivers had mild anxiety with less than 17 score.
Conclusion: Most of the caregivers were anxious due to congenital lower limb deformities of their children.
Keywords: anxiety level; caregivers; congenital lower limb deformities; developmental dysplasia of hip; leg length discrepancy
Introduction
Congenital lower limb deformities impose substantial physical, emotional and financial challenges not only on affected children but also on their families [1]. Congenital Malformations account for approximately 2%-4% of live births across the globe with limb defects representing a notable subset that can result in lasting disability and complications for rehabilitation [2]. Numerous studies emphasize the psychological impact of caring for a child with congenital anomalies, with anxiety prevailing among primary caregivers. A prospective study of parents managing congenital clubfoot treated with the Ponseti method revealed significant depression, stress, and anxiety specifically among highly educated mothers although symptoms were declining with treatment [3].
In the case of congenital pseudarthrosis of the tibia, caregivers also exhibited significantly higher anxiety and depressive symptoms compared to those caring for unaffected children-factors that may influence the child’s behavioral outcomes and long-term rehabilitation [4]. A scoping review on caregivers of children with lower limb amputations highlighted that psychological support was among the most persistent apprehensions as caregivers were more prone to experience depressive symptoms, anxiety and irritability that directed towards the need for psychological counselling, and organized institutional support [5].
A cross-sectional survey from Northwestern Pakistan (2017-2021) among 141 cases with congenitally deformed limbs explored that there was heterogeneity in defect types (transverse, longitudinal, intercalary). Moreover, multifactorial etiology was identified with prime attribution to parental consanguinity [6]. Likewise, a multicenter study carried out among residents of Peshawar revealed that limb abnormalities constituted around 26% of all congenital malformations [7]. Similarly, a survey among cohort of 1185 cases from Baluchistan with congenital malformations illustrated that one percent of it is sporadic while 51% of deformations were linked with consanguineous marriages [8]. A mixed method study by Saeed S et al at a tertiary care hospital of Karachi emphasized the multi-faceted aspect of burden related to caregivers of hereditary pediatric illnesses [9]. The caregivers of disabled children were subjected to multiple challenges like joblessness, depression and poor quality of life [10].
The psychological burden among caregivers of children with congenital anomalies seems to be a real and unmet need; yet this issue needs methodical study. In the light of this research gap, the present study is intended to investigate the anxiety levels among caregivers of children with congenital lower limb deformities in Pakistan. This study would provide actionable data to inform healthcare providers, policymakers, and rehabilitation services for paying attention to psychosocial needs apart from physical care. This study would facilitate designing responsive, compassionate and holistic care pathways to support the children with physical deformities as well as their families.
Methods
A cross-sectional descriptive study was carried out among 100 caregivers of the children who were diagnosed with lower limb deformities at Benazir Bhutto Hospital Rawalpindi and were enrolled in the study through purposive non-probability sampling. This study was done in the partial fulfillment of BSc (Hons) Orthotics & Prosthetics degree at Informed consent was taken from all the caregivers for data collection. The responses were gathered from caregivers of the children by using Standardized Hamilton Anxiety Rating Scale (HAM-A). This scale is among the extensively used scales to clinically measure the severity of anxiety. It comprises of 14 items with scoring of each item varying from 0-4 (0=not present, 4=severe). In this way, minimal score = 0 and highest score = 5611.
This scale encompasses two domains that include psychic (mental) and somatic (physical). Items related to psychic domain are anxious mood, tension, fears, insomnia, memory and depressed mood. Items pertaining to somatic domain are sensory and muscular symptoms, cardiovascular, respiratory, gastrointestinal, genitourinary, autonomic symptoms and behavior at interview. The cut-off levels for interpreting the scores of HAM-A rating scale are illustrated below:
- 0-17: Mild
- 18-24: Mild to Moderate
- 25-30: Moderate to Severe
- 30: Very Severe [12]
This scale has been verified as having good reliability and concurrent validity particularly among anxious and depressed cases [11]. However, its inter-rater reliability and construct validity was determined to be more in acceptable range among adolescents [13]. Data was entered and analyzed by using SPSS version 25 and MS Excel 2019. Descriptive statistics were applied.
Results
Of the 100 caregivers of the patients with congenital lower limb deformities enrolled in the study, 56 were males while 44 were females. Mean age of the respondents was 21.7 ± 9.2 years. Most (21%) of the patients with lower limb deformity had DDH as shown below in Figure 1.
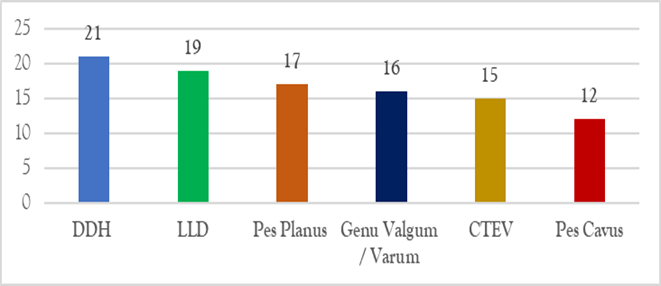
Figure 1: Types of Congenital lower limb deformities among patients.
Majority (67%) of the care givers were determined to have mild to moderate anxiety as depicted below in Figure 2.
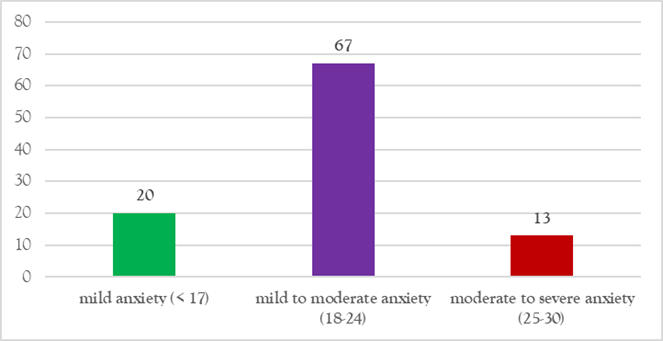
Figure 2: Mild to moderate anxiety, moderate to severe anxiety.
Discussion
Of the 100 children discussed in present study with congenital lower limb deformities, 44% and 56% were females and males respectively. Contrary to our result, data from a book revealed occurrence of one of the lower limb deformities that is DDH more among females in female: male as 6:1. This discrepancy was linked with gender-wise hormonal and anatomical diversities [14]. Contrary to this, a hospital-based descriptive study done among cases of Khyber Pakhtunkhwa presented the congenital occurrence of club foot among 210 males and 104 females [15]. Similarly, an Indian study by Barik S et al reflected the higher prevalence of lower limb deformities particularly Congenital Talipes Equinovarus (CTEV) among males [16]. Apart from gender-based differences, other socio-demographic and environmental aspects should also be studied while developing association of lower limb deformity with an entity. Systematic reviews and meta-analysis cane help us to great extent in establishing the relevant causal association.
Most (21%) of the children in present study had DDH followed by LLD (19%). Overall DDH has been diagnosed among 1-1.5 infants / 100 births across the globe but some regional disparities in its prevalence have also been documented [17]. A systematic review and meta-analysis done by Tao Z et al showed occurrence of Developmental Dysplasia of Hip among 1 in 100 female infants. However, recommendation was to promote routine screening among infants for avoiding complex developmental disorders [18]. On the other hand, a retrospective cross-sectional survey spanning over 5 years (2018-2023) demonstrated 0.50% prevalence of DDH [19]. A similar study carried out by Marvi N et al among infants of Karachi revealed higher incidence of DDH among males (16.08%) than those of females (14.78%) although gender-based disparity was statistically insignificant. Moreover, ethnic variation was quite prominent with more Sindhi infants diagnosed with pathological hips (9.13%) than those of Punjabi (7.39%) and Pathan (6.08%) [20]. Apart from nation-wide discrepancy, ethnic variation is also a noteworthy dimension that should further be scrutinized by community screening primarily at massive scale.
Of the 100 children mentioned in our study with congenital lower limb deformities, 19 were diagnosed cases of Leg Length Discrepancy (LLD). Being a deformity secondary to club foot, a retrospective study by Schaibley C et al, around 14.4% of clubfoot children treated through ponseti casting had LLD [21]. Consistent with these findings, a retrospective cohort study revealed 9% LLD among club foot cases and 23% of them had unilateral clubfoot deformity [22]. The association of LLD with DDH have also been determined by some researchers, therefore a study by Merchant RM et al concluded that meticulous observation of LLD with DDH is markedly needed for appropriate management of the cases [23]. Inclusion of genetics in occurrence of DDH is in dire need of further comprehensive studies [24]. Pes planus is another lower limb deformity that has remarkably been detected among children whose caregivers responded in present study. It has frequently been reported among Pakistani children. Its prevalence among children of Lahore was found to be 40.6% [25]. However, prevalence of pes planus was comparatively less among students of Karachi (15.5%) [26] and those belonging to Rawalpindi and Islamabad (14.8%) [27]. Substantial variations in deformities have been witnessed even among different cities of Pakistan. The underlying etiology demands digging out of real-time evidence. This will definitely prove beneficial for the community as meticulous supervision of the cases would enable the stakeholders to take necessary rehabilitative measures.
About 67 percentage caregivers of the children with congenital lower limb deformities had mild to moderate anxiety in the current study. A comparative cross-sectional study carried out on a large scale by Yu Y et al was illustrative of higher rates of anxiety among parents and relatively more burden than the parents of healthy children [28]. The parents of children with known DDH were quite apprehensive and depressed at the time of diagnosis but later anxiety level dropped when they learned to manage their children with this deformity [29]. Likewise, according to a prospective study, depression, anxiety and stress among caregivers of children with clubfoot was substantially declined after ponseti casting of their affected children. Although parents of affected children were much disturbed psychologically but initiation of treatment and awareness about managing lower limb deformities considerably relieved their anxiety. Hence, pre- and post-management psychological well-being of the caregivers should be given due consideration for the mitigating their depressiveness [30]. According to a prospective cohort study by Mahan MT et al meeting of the caregivers with pediatric orthopedic surgeon can momentously relieve their anxiety [31], so this initiative along with prenatal counseling can help a great deal to cope up with existing scenario. One of the limitations of this study was small sample size and short duration of study. Planning a multi-center study particularly gathering responses from caregivers of affected children from both public and private sector can prove quite insightful and enlightening for the stakeholders.
Conclusion & Recommendations
Majority of the patients having children with congenital lower limb deformities were identified with mild to moderate anxiety. Proper counseling of the parents can prove beneficial in mitigating the frequency of anxiety and stress. Moreover, it was suggested to organized awareness campaigns and seminars for such parents that will not only encourage them to improve their quality of life but will also enable them to manage the stress associated with deformity of their children.
List of Abbreviations
CTEV: Congenital Talipes Equinovarus
DDH: Developmental Dysplasia of Hip
LLD: Leg length Discrepancy
HAM-A: Hamilton Anxiety
Declarations
Conflicts of Interest
The authors declared no conflict of interest.
Source of Funding
The author(s) received no financial support for the research, authorship and or publication of this article.
References
- Zhuang T, El-Banna G, Frick S. (2019). Arthrodesis of the Foot or Ankle in Adult Patients with Congenital Clubfoot. Cureus. 11(12):e6505.
Publisher | Google Scholor - Bibi A, Uddin S, Naeem M, Syed A, Ud-Din Qazi W, et al. (2023). Prevalence pattern, phenotypic manifestation, and descriptive genetics of congenital limb deficiencies in Pakistan. Prosthet Orthot Int. 47(5):479-485.
Publisher | Google Scholor - Özdemir MA, Topak D, Turgut C, Telek M, Dogar F. (2022). Evaluation of depression, anxiety, and stress status in parents of patient with congenital clubfoot treated with Ponseti method: A prospective study. Medicine (Baltimore). 101(44):e31654.
Publisher | Google Scholor - Xie JH, Mei HB, Liu K, Zhu GH, Ouyang YQ, et al. (2022). Analysis of related factors of behavioral problems in children with congenital pseudarthrosis of tibia. Rev Assoc Med Bras (1992). 68(7):893-897.
Publisher | Google Scholor - Rodrigues D, Silva R, Castanheira S, Carvalho L, Pinto C. (2024). Needs of Family Caregivers of People with Lower Limb Amputations: A Scoping Review. Behavioral Sciences. 14(4):326.
Publisher | Google Scholor - Bibi A, Uddin S, Naeem M, Syed A, Ud-Din Qazi W, et al. (2023). Prevalence pattern, phenotypic manifestation, and descriptive genetics of congenital limb deficiencies in Pakistan. Prosthet Orthot Int. 47(5):479-485.
Publisher | Google Scholor - Naqvi SF, Ameena U, Qazi WU, Ahmad S, Iqbal A, et al. (2024). Burden of congenital and hereditary anomalies and their epidemiological attributes in the pediatric and adult population of Peshawar valley, Pakistan. Pak J Med Sci. 40(10):2181-2189.
Publisher | Google Scholor - Azmatullah, Khan MQ, Jan A, Mehmood J, Malik S. (2024). Prevalence-pattern of congenital and hereditary anomalies in Balochistan Province of Pakistan. Pak J Med Sci. 40(9):1898-1906.
Publisher | Google Scholor - Saeed S, Malik MGR, Khan MH, Malik SAR, Aziz B. (2024). Care for the caregiver: an exploration of caregiver burden of children with chronic medical conditions at a tertiary care hospital in Karachi, Pakistan - a mixed-methods study. BMJ Open. 14(5):e083088.
Publisher | Google Scholor - Qayyum A, Lasi S, Rafique G. (2013). Perceptions of primary caregivers of children with disabilities in two communities from Sindh and Balochistan, Pakistan. Disability CBR & Inclusive Development, 24(1):130-142.
Publisher | Google Scholor - Maier W, Buller R, Philipp M, Heuser I. (1988). The Hamilton Anxiety Scale: reliability, validity and sensitivity to change in anxiety and depressive disorders. J Affect Disord, 14(1):61-68.
Publisher | Google Scholor - Zimmerman M, Martin J, Clark H, McGonigal P, Harris L, et al. (2017). Measuring anxiety in depressed patients: A comparison of the Hamilton anxiety rating scale and the DSM-5 Anxious Distress Specifier Interview. J Psychiatr Res, 93:59-63.
Publisher | Google Scholor - Clark DB, Donovan JE. (1994). Reliability and validity of the Hamilton Anxiety Rating Scale in an adolescent sample. J Am Acad Child Adolesc Psychiatry, 33(3):354-360.
Publisher | Google Scholor - Qin S, Shi L, Guo B, Jiao S, Zang J. (2024). Congenital deformity of lower limbs. In: Guo B, Huang P, editors. Atlas of Limb Deformity. Singapore: Springer, 21-61.
Publisher | Google Scholor - Muhammad B, Aftab A, Kamran M, Saqulain G. (2023). Occurrence and pattern of clubfoot deformity in Khyber Pakhtun Khwa: Hospital based physical rehabilitation center perspective. RMJ, 48(4):889-892.
Publisher | Google Scholor - Barik S, Pandita N, Paul S, Kumari O, Singh V. (2021). Prevalence of congenital limb defects in Uttarakhand state in India - A hospital-based retrospective cross-sectional study. Clinical Epidemiology and Global Health, 9: 99-103.
Publisher | Google Scholor - Alanazi ZA, Alshammari AM, Alruwaili RM, Alnasser RM, Alkhalifah HN, et al. (2025). Prevalence of developmental dysplasia of the hip in Al Jouf province, Saudi Arabia. World J Orthop. 16(6):107423.
Publisher | Google Scholor - Tao Z, Wang J, Li Y, Zhou Y, Yan X, et al. (2023). Prevalence of developmental dysplasia of the hip (DDH) in infants: a systematic review and meta-analysis. BMJ Paediatr Open, 7(1):e002080.
Publisher | Google Scholor - Alanazi ZA, Alshammari AM, Alruwaili RM, Alnasser RM, Alkhalifah HN, et al. (2025). Prevalence of developmental dysplasia of the hip in Al Jouf province, Saudi Arabia. World J Orthop. 16(6):107423.
Publisher | Google Scholor - Marvi N, Khokhar SM, Qamar A, Ashfaq M. (2024). Association of hip dysplasia in newborns with ethnicity using graf method ultrasound. Pakistan Journal of Medical Sciences, 41(1):247-250.
Publisher | Google Scholor - Schaibley C, Torres-Izquierdo B, Siddabattula R, Hosseinzadeh P. (2025). Prevalence and Risk Factors for Leg Length Discrepancy in Children With Idiopathic Clubfoot Treated With Ponseti Method. J Pediatr Orthop, 45(4):234-238.
Publisher | Google Scholor - Addar A, Bouchard M. (2022). Clinically Detected Leg Length Discrepancy in Patients With Idiopathic Clubfoot Deformity: Prevalence and Outcomes. J Pediatr Orthop, 42(7):e772-e776.
Publisher | Google Scholor - Merchant RM, Tolk JJ, Ayub AA, Eastwood DM, Hashemi-Nejad A. (2022). The Importance of Monitoring and Factors That May Influence Leg Length Difference in Developmental Dysplasia of the Hip. Children (Basel). 9(12):1945.
Publisher | Google Scholor - Jacobsen KK, Laborie LB, Kristiansen H, Schäfer A, Gundersen T, et al. (2024). Genetics of hip dysplasia - a systematic literature review. BMC Musculoskelet Disord. 25(1):762.
Publisher | Google Scholor - Ateeque A, Shabbir S, Nadeem T, Zubair H, Khizar Z. (2024). Prevalence of flatfoot in school-going children, Lahore. Journal of Health and Rehabilitation Research, 4(2):745-749.
Publisher | Google Scholor - Ahmed A, Ahmed S. (2019). Prevalence of flatfoot among young adults and its relation with body mass index. RMJ, 44(3):644-645.
Publisher | Google Scholor - Ali M, Asadullah M, Amjad I. (2013). Prevalence of flatfoot in 6-10 years old school going children. Rawal Med J, 38:385-387.
Publisher | Google Scholor - Yu Y, Yang L, Liu Y, Fang J, Wang H, et al. (2025). Caregiver burden and associated factors among primary caregivers of children with congenital disorders: a comparative cross-sectional study in Hunan Province, China. BMC Nurs, 24:491.
Publisher | Google Scholor - Ali DMSP, Shaikh KA, Jamali AG, Maitlo AA, Ali M. (2024). Effects on Parental Mental Health after Diagnosis and Treatment of Developmental Dysplasia of the Hip (DDH). Journal of Pakistan Orthopaedic Association, 36(4):200-206.
Publisher | Google Scholor - Özdemir MA, Topak D, Turgut C, Telek M, Dogar F. (2022). Evaluation of depression, anxiety, and stress status in parents of patient with congenital clubfoot treated with Ponseti method: A prospective study. Medicine (Baltimore). 101(44):e31654.
Publisher | Google Scholor - Mahan ST, Miller PE, May CJ, Kasser JR. (2019). Prospective evaluation of parental anxiety related to newborn foot disorder. J Child Orthop, 13(5):500-507.
Publisher | Google Scholor























