

Case Report
An Interesting Presentation of The Bezold-Jarisch Reflex Following an Iatrogenic Intestinal Perforation: A Case Report
- Sultan Akbar
- Phillip Tran
- Leonard B. Goldstein *
A.T. Still University, School of Osteopathic Medicine in Arizona, Mesa, United States America.
*Corresponding Author: Leonard B. Goldstein, A.T. Still University, School of Osteopathic Medicine in Arizona, Mesa, United States America.
Citation: Akbar S, Tran P, Goldstein LB. (2026). An Interesting Presentation of The Bezold-Jarisch Reflex Following an Iatrogenic Intestinal Perforation: A Case Report, International Clinical and Medical Case Reports, BioRes Scientia Publishers. 5(2):1-4. DOI: 10.59657/2837-5998.brs.26.063
Copyright: © 2026 Leonard B. Goldstein, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: May 20, 2026 | Accepted: June 05, 2026 | Published: June 12, 2026
Abstract
Colonoscopies are considered a necessary screening procedure for patients typically starting at 45 years of age. The patients are notified that there is a risk of intestinal perforation, however this is unlikely. When intestinal perforations occur, the standard emergency surgency is a colonic resection. The patient is monitored thereafter and no other procedural protocols exist for the patient’s treatment. When the patient begins to experience conduction blocks and heart rhythm abnormalities, further consideration must be given for potential repercussions of the perforation. We present the case of a patient who suffered from an iatrogenic intestinal perforation that began to experience the Bezold-Jarisch reflex.
Keywords: bezold-jarisch reflex; pacemaker; perforation; conduction block
Introduction
Colorectal cancer (CRC) remains a major global health burden, with more than 1.9 million new cases and over 900,000 deaths estimated worldwide in 2022 [1]. Screening is central to CRC prevention because early detection and removal of premalignant lesions can reduce CRC incidence and mortality [2]. Current United States Preventive Services Task Force recommendations support screening for colorectal cancer in adults aged 45 to 75 years, with individualized decision-making in select older adults [3]. Colonoscopy is widely recognized as a gold standard modality for colorectal cancer screening and diagnosis, and it also serves as a therapeutic intervention through biopsy and polypectomy of lesions with malignant potential [4].
Despite its diagnostic and therapeutic value, colonoscopy is associated with rare but serious complications. Colonoscopic perforation (CP) is one of the most severe adverse events following lower gastrointestinal endoscopy and may result in peritonitis, sepsis, emergency surgery, prolonged hospitalization, and increased mortality [5]. Reported perforation rates vary according to whether the procedure is diagnostic or therapeutic, with higher risk during interventions such as polypectomy, dilation, or endoscopic mucosal resection [5,6]. Management depends on the patient’s clinical stability, bowel preparation, perforation size and location, degree of contamination, and timing of recognition [6]. When operative intervention is required, surgical management may include primary repair, resection with anastomosis, or resection with ostomy, performed through either laparoscopic or open techniques [7].
The Bezold–Jarisch reflex (BJR) is an inhibitory cardiovascular reflex mediated by vagal afferent fibers and characterized by increased parasympathetic activity with reduced sympathetic tone [8]. Clinically, this reflex may manifest as bradycardia, hypotension, apnea, atrioventricular block, or, in severe cases, asystole [8,9]. Although the BJR has classically been described in settings such as myocardial ischemia, anesthesia, hypovolemia, and pharmacologic stimulation, it has also been reported in association with procedural and perioperative events [9,10]. More recently, BJR-induced cardiac arrest has been described during colonoscopy under sedation, highlighting the potential relevance of this reflex in gastrointestinal procedural settings [11].
This article presents the unusual case of a patient who suffered an iatrogenic intestinal perforation during a routine colonoscopy. His postoperative recovery was subsequently complicated by significant cardiac conduction abnormalities that were attributed to the Bezold-Jarisch reflex.
Case Presentation
The patient was a male in his 60s with a past medical history significant for hypertension and prostate cancer. Early in the year 2024 he was seen by his primary care physician for an annual follow-up. He had no complaints and was informed that he was overdue for a colonoscopy. While reluctant at first, later that year he proceeded with the colonoscopy.
2 days after his colonoscopy he presented to the emergency room complaining of worsening abdominal pain and a 2-day history of constipation. He identified pain in all 4 quadrants of the abdomen and felt that it was worsening. The emergency department then ordered a CT of the Abdomen and Pelvis with contrast (Figure 1).
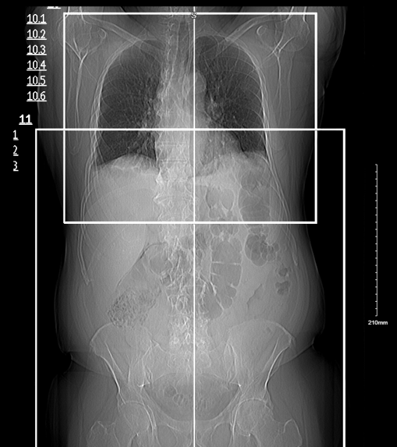
Figure 1: CT of the Abdomen and Pelvis with Contrast which the patient received at the emergency room.
There was multiple dilated fluid filled loops of small bowel throughout the abdomen most consistent with adynamic ileus. No small bowel obstruction was evident. A large volume of free air was present within the abdomen suggesting perforation.
The emergency department physician then consulted the general surgeon on call who believed the patient’s elevated white blood cell count and CT findings were concerning for both an ischemic colon and pneumoperitoneum. The formal diagnosis of perforation ischemia at the hepatic flexure was given to the patient. The surgeon proceeded to perform an exploratory laparotomy extended right hemicolectomy with primary anastomosis abdominal washout.
The patient was then hospitalized and followed by a general surgeon and hospitalist. His ileus began to resolve, and his recovery initially showed promise. However, cause for concern began to arise on postoperative day #4, when the patient began to have bradycardia with a heart rate near 28 BPM, pauses, and dropped p-waves. The most concerning EKG showed a left bundle branch block with a right ventricular conduction delay (Figure 2).
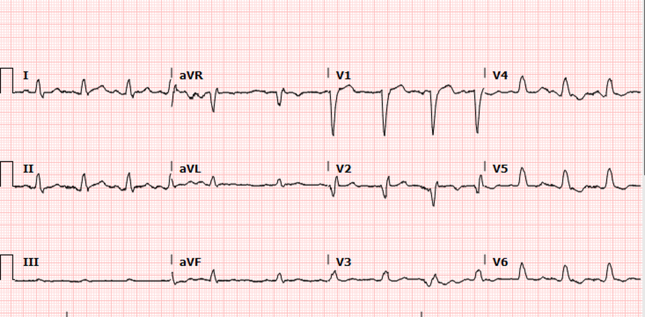
Figure 2: Concerning EKG that the patient had on postoperative day #4.
The cardiology team was then consulted, and the doctor’s impression was that the patient was having symptomatic sinus pauses. The patient was taking thorazine, so the cardiologist discontinued it as it may have contributed to this. Also, the cardiologist wanted the patient to be monitored on telemetry, have an echocardiogram, and have a transvenous temporary pacemaker insertion.
The transthoracic echocardiogram showed a normal left ventricular cavity size with a normal systolic function (Figure 3). The estimated ejection fraction was 60%. Furthermore, the transvenous pacemaker insertion was successful and the patient’s telemetry showed a normal heart rhythm and rate. Incidentally, the patient began to report that he was also having progressively worsening dysphagia. The patient also was noted to have several apneic spells within the night, in which there was a drop in oxygen saturations down to about 80%. The cardiologist at the time began to suspect that the patient’s cardiac conduction block was a result of the Bezold-Jarisch Reflex, in which the vagal nerve fibers were potentially stimulated during the iatrogenic perforation of the small bowel, which inevitably lead to increased vagal output. This explained the patient’s conduction block, apneic spells, dysphagia, and bradycardia.
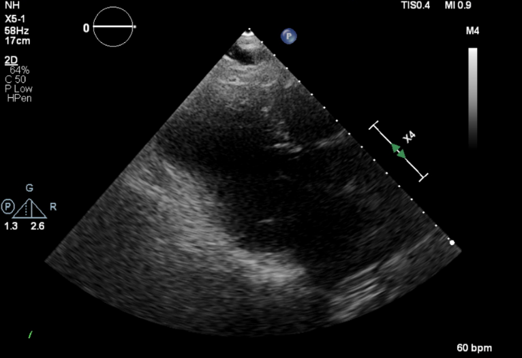
Figure 3: Normal transthoracic echocardiogram that the patient had.
Discussion
To start, a perforation is a very rare consequence of a colonoscopy. Further underlying connective tissue disease, or if the cause of the perforation was due to the gastroenterologist’s technique. The cardiac conduction block that the patient later experienced seems to be part of the Bezold-Jarish Reflex and resulted in quite significant suffering. Consideration for this reflex should definitely be adopted into the standard protocol for handling a patient that has incurred an iatrogenic perforation. If the physician did not realize that this was a temporary reflex that the patient was having, the patient could have been left with a permanent pacemaker. Future physicians would not have looked deep into the reasons for the patient’s pacemaker and the patient would have had a significant hardship and decreased quality of life. The patient had such a significant event, this outcome must be more well-established within the literature as occurring after an iatrogenic perforation. If the patient did not come into the emergency room as he did, he could have died. It is fortunate that the general surgeon was able to perform the hemicolectomy with a primary anastomosis otherwise the patient could have had an ostomy bag for the rest of his life as well. This case also elucidates the importance of considering seemingly outlandish causes for presentations. Medicine has many intricacies and a patient's condition can include many moving parts. It is important for a physician to recognize this and refrain from becoming complacent, despite how routine things may seem at times.
Conclusion
Colonoscopies are a necessary part of a person’s annual screening for illness. Perforation is a known but rare complication of a colonoscopy and is seldom a reason for a patient to defer it. When a patient with a significant gastrointestinal complaint later presents with a cardiac conduction block, physicians must make sure to keep the Bezold-Jarisch reflex in mind when contemplating the patient’s diagnosis. Further research is necessary to better understand the underlying pathophysiology of this reflex and what precautions could be taken to ensure that a patient undergoing a procedure does not develop this condition.
Statement of Informed Consent
Informed consent was obtained from the patient that was presented in the case report.
References
- Bray, F., Laversanne, M., Sung, H., Ferlay, J., Siegel, R. L., et al. (2024). Global Cancer Statistics 2022: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA: A Cancer Journal for Clinicians, 74(3):229-263.
Publisher | Google Scholor - Jayasinghe, M., Prathiraja, O., Caldera, D., Jena, R., Coffie-Pierre, J. A., et al. (2023). Colon Cancer Screening Methods: 2023 Update. Cureus, 15(4).
Publisher | Google Scholor - US Preventive Services Task Force, Davidson, K. W., Barry, M. J., Mangione, C. M., Cabana, M., et al. (2021). Screening for Colorectal Cancer: Us Preventive Services Task Force Recommendation Statement. JAMA, 325(19):1965-1977.
Publisher | Google Scholor - Dsouza Royson, Gopal Menon, Christopher Pfeifer. (2025). Colonoscopy. StatPearls [Internet]. StatPearls Publishing.
Publisher | Google Scholor - Lohsiriwat, V. (2010). Colonoscopic Perforation: Incidence, Risk Factors, Management and Outcome. World Journal of Gastroenterology: WJG, 16(4):425.
Publisher | Google Scholor - de’Angelis, N., Di Saverio, S., Chiara, O., Sartelli, M., Martínez-Pérez, A., et al. (2018). 2017 WSES Guidelines for The Management of Iatrogenic Colonoscopy Perforation. World Journal of Emergency Surgery, 13(1):5.
Publisher | Google Scholor - Thompson, E. V., Snyder, J. R. (2019). Recognition and Management of Colonic Perforation Following Endoscopy. Clinics in Colon and Rectal Surgery, 32(03):183-189.
Publisher | Google Scholor - Mark, A. L. (1983). The Bezold-Jarisch Reflex Revisited: Clinical Implications of Inhibitory Reflexes Originating in The Heart. Journal of the American College of Cardiology, 1(1):90-102.
Publisher | Google Scholor - Hossain, N., Hossain, N., Al-Sadawi, M., Haq, S. (2020). Bezold–Jarisch Reflex-Mediated Asystole During Dobutamine Stress Testing: A Case Report. European Heart Journal-Case Reports, 4(6):1-6.
Publisher | Google Scholor - Kirsch, C., Badwal, A., Rabany, R., Shabanian, J., Dormer, C. L., et al. (2024). Bezold-Jarisch Reflex Presenting with Bradypnea, Bradycardia, and Hypotension Following Combined Spinal Epidural Prior to Cesarean Section: A Case Report. Cureus, 16(2).
Publisher | Google Scholor - Liu, Q., Jia, S., Chen, H., Liu, H., Xu, L., et al. (2025). Bezold-Jarisch Reflex-Induced Cardiac Arrest During Colonoscopy Under Sedation: A Case Report. The American Journal of Case Reports, 26:e949496.
Publisher | Google Scholor























