

Case Report
Abnormal EKG Leading to Coronary Artery Bypass Graft in A Patient Seeking Cataract Surgery Clearance: A Case Report
A.T. Still University, School of Osteopathic Medicine in Arizona, Mesa, United States America.
*Corresponding Author: Leonard B. Goldstein, A.T. Still University, School of Osteopathic Medicine in Arizona, Mesa, United States America.
Citation: Akbar S, Tran P, Goldstein LB. (2026). Abnormal EKG Leading to Coronary Artery Bypass Graft in A Patient Seeking Cataract Surgery Clearance: A Case Report, Journal of Clinical Research and Clinical Trials, BioRes Scientia Publishers. 5(2):1-5. DOI: 10.59657/2837-7184.brs.26.070
Copyright: © 2026 Leonard B. Goldstein, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: May 27, 2026 | Accepted: June 25, 2026 | Published: July 03, 2026
Abstract
A cataract surgery is a regular routine surgery that many patients end up needing. It is not uncommon for a surgeon to request cardiac clearance for a surgery. While many patients likely end up having an unremarkable EKG, a number of patients have an abnormal EKG. Some patients with abnormal EKGs might not have any cardiovascular symptoms. Following an ischemic cardiac work-up, some patients are left with the surprise of needing a coronary artery bypass graft due to significant coronary artery disease. We present the case of a 61-year-old male who was found to have an abnormal EKG. A subsequent ischemic work-up indicated that he had a left main coronary artery 95% occluded and needed an urgent coronary artery bypass graft. It was important to use his cardiac risk factors to guide his treatment as compared to the characteristic symptoms he seemed to lack.
Keywords: cataract surgery; abnormal EKG; coronary artery disease; cardiac stress test; myocardial infarction
Introduction
Cataracts are the world’s leading cause of remediable blindness [1]. While some cataracts may be congenital, secondary to trauma, or drug-induced, most cataracts are age-related [1]. Cataract surgery is the most effective and currently the only approved intervention for cataracts regardless of etiology [1]. Cataract surgery is generally considered a low-risk noncardiac procedure, and routine preoperative medical testing in asymptomatic patients has not consistently been shown to improve perioperative outcomes [2]. However, when abnormal cardiovascular findings are identified during preoperative evaluation, further cardiac assessment may be clinically appropriate, particularly in patients with significant risk factors for coronary artery disease.
Many patients undergoing major noncardiac and vascular surgery are at risk for a major adverse cardiac event (MACE) [3]. In the United States, millions of patients undergo noncardiac surgery annually, and a subset experience postoperative myocardial infarction or other cardiovascular complications [3]. To minimize perioperative complications and reduce morbidity and mortality, a thorough preoperative evaluation of patients with known or suspected heart disease, along with appropriate risk stratification, is necessary [3]. Contemporary perioperative cardiovascular guidelines emphasize a stepwise approach that incorporates surgical risk, patient-specific cardiovascular risk factors, functional capacity, active cardiac conditions, and whether additional testing would change management [4].
Asymptomatic coronary artery disease (ACAD) is a significant diagnosis documented in the cardiology literature [5]. This syndrome is characterized by myocardial ischemia without typical anginal pain [5]. Silent myocardial ischemia is defined by objective evidence of myocardial ischemia in the absence of angina or anginal equivalents and may be detected through electrocardiography, ambulatory monitoring, exercise stress testing, stress imaging, or coronary evaluation [6]. Risk factors for silent myocardial ischemia overlap with those for symptomatic coronary artery disease and include hypertension, diabetes mellitus, smoking, hyperlipidemia, obesity, physical inactivity, and family history of heart disease [7]. Diagnosis must therefore be specific and supported by objective evidence of ischemic change rather than symptoms alone [5,6].
ACAD appears to occur in three different types of individuals [5]. A type 1 person is totally asymptomatic, has no history of angina, myocardial infarction, or congestive heart failure, and demonstrates myocardial ischemia [5]. The type 2 patient with ACAD is in the post-myocardial infarction period and demonstrates asymptomatic myocardial ischemia [5]. The type 3 patient with ACAD is one who experiences myocardial ischemia both with and without pain [5]. When ischemic evaluation reveals significant left main coronary artery disease, coronary artery bypass grafting is recommended to improve survival in appropriate patients [8].
This case report presents an asymptomatic patient undergoing preoperative evaluation for cataract surgery who was found to have an abnormal EKG, a positive ischemic workup, and severe left main coronary artery stenosis requiring urgent coronary artery bypass grafting.
Case Presentation
The patient was a 60-year-old male with a past medical history significant for hypertension that was undergoing an EKG prior to having a cataracts surgery. The EKG was abnormal showing sinus tachycardia with occasional supraventricular premature complexes, an incomplete right bundle branch block, and a septal myocardial infarction of indeterminate age (Figure 1). The patient was then referred to a cardiologist for further evaluation. He presented to the cardiology clinic with a blood pressure of 199/105 mmHg despite being compliant with his lisinopril 40mg daily. He denied any cardiovascular symptoms such as dyspnea on exertion, shortness of breath, syncope, presyncope, or palpitations. Amlodipine 5mg was added to his treatment regimen and the patient was to follow-up in the clinic 2 weeks later after a nuclear stress test.
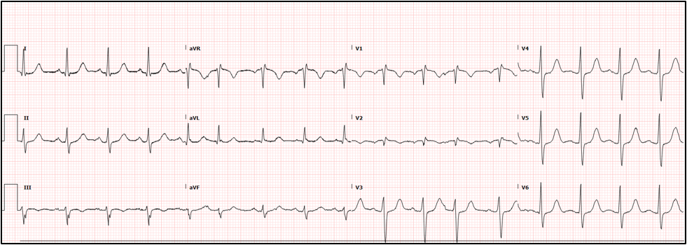
Figure 1: Abnormal preoperative EKG that the patient had.
The patient presented two weeks later for a follow-up after an abnormal stress test (Figure 2). The treadmill stress test showed 3 mm horizontal, downsloping distal few ST depression with hypotension indication for positive EKG for ischemia. Myocardial perfusion imaging showed a small inferior wall reversible defect with dilated 3 times daily 1.33 indicating possible extensive CAD. LVEF also dropped during stress. At this point the patient needed coronary artery interrogation with an angiogram. The patient voiced understanding and agreed to proceed with left heart cath. With possible advanced CAD on a nuclear stress test, the patient was strongly advised to be admitted to the hospital the same day, but refused. The patient was then scheduled a coronary angiogram and given precautions on when to present to the emergency room.
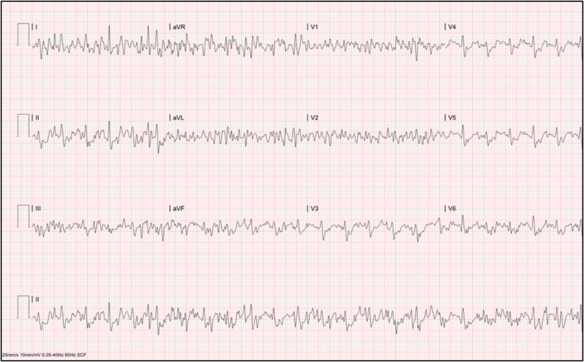
Figure 2: Treadmill stress test that was positive for ischemia that the patient had.
The patient then presented to the emergency room the next day with increased anxiety following the abnormal treadmill stress test. He denied any chest pain, palpitations, dyspnea, dizziness, syncope, or presyncope. He still received an expedited coronary angiogram which showed 95% stenosis of the left main coronary artery, 50% stenosis of the left anterior descending artery, and 55% stenosis of the first diagonal (Figure 3). The patient was then referred to cardiothoracic surgery for an urgent CABG and was placed on intravenous heparin and metoprolol.

Figure 3: Coronary angiogram the patient had showing significant left coronary artery stenosis.
The patient then underwent a triple coronary bypass grafting with an endoscopic saphenous vein harvesting. The procedure was performed without difficulties, and a follow-up chest x-ray was performed (Figure 4). The chest x-ray showed a right internal jugular central venous catheter present with the tip over the superior vena cava. Mediastinal drains were present without visible pneumothorax. Lung volumes were low and there was mild bibasilar atelectasis. No pleural effusions were identified.
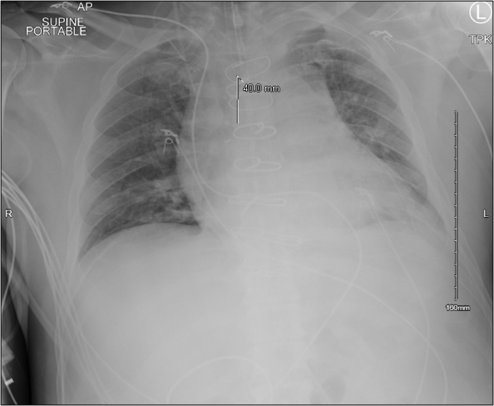
Figure 4: Postoperative chest x-ray that the patient had.
The patient was then started on aspirin, plavix, atorvastatin, and low-dose metoprolol with vital signs within normal ranges. The patient was then offered a nutritional evaluation to make lifestyle changes for a better outcome. Following an uncomplicated post-surgical stay in the cardiac intensive care unit, the patient was then discharged within a week. Three weeks later, the patient presented to an outpatient cardiology follow-up appointment with vital signs within normal ranges. After having an EKG showing normal sinus rhythm with a moderate intraventricular conduction delay, the patient received cardiac clearance to have his cataract surgery (Figure 5).
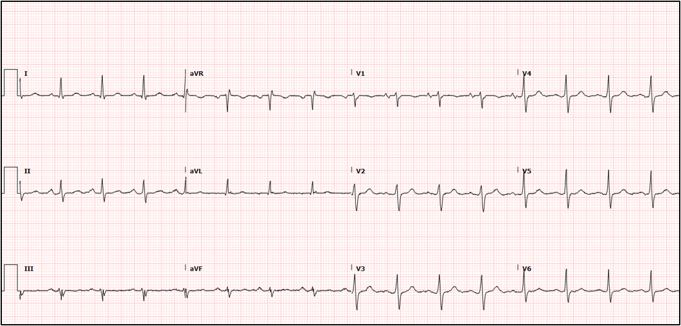
Figure 5: Normal EKG the patient had at his hospital follow-up.
Discussion
The patient initially presented to the cardiologist for the cardiac clearance for his cataract surgery. He had no outstanding cardiovascular complaints but had a lifetime smoking history and hypertension. After a positive stress test, it was revealed that he had 95% occlusion of the left main coronary artery. He could have dropped dead without any symptoms with an artery that occluded. Had the doctor not advised him to go to the emergency room, he likely could have died. This case highly accentuates the importance of risk factors for someone having coronary artery disease, and just that a patient doesn’t have symptoms should exclude them from having an ischemic workup when an EKG is abnormal. Had the ophthalmologist not requested a cardiac clearance for the cataract surgery, there is a chance that the patient could have died under anesthesia, without anybody knowing that there was any underlying coronary artery disease.
Conclusion
Cataract surgery is a common surgery performed on patients. It is very common for a surgeon to request a cardiac clearance. It is important significant efforts are made to ensure the patient does not have any adverse events under anesthesia, and in this case the patient’s life was likely saved. Had the patient not received an ischemic workup for an abnormal EKG, the patient could have died at any time. It was also important for the cardiologist to prioritize the patient’s risk factors for coronary artery disease over the symptoms in this case and advise the patient to present to the emergency room where a 95% occlusion was found. Further research must be made into better understanding asymptomatic coronary artery disease and diagnosing it early on. Doctors must be kept well-informed of how important risk factors are in screening someone for coronary artery disease.
Statement of Informed Consent
Informed consent was obtained from the patient that was presented in the case report.
References
- Moshirfar, M., Milner, D., Patel, B. C. (2023). Cataract Surgery. In: StatPearls. StatPearls Publishing.
Publisher | Google Scholor - Schein, O. D., Katz, J., Bass, E. B., Tielsch, J. M., Lubomski, L. H., et al. (2000). The Value of Routine Preoperative Medical Testing Before Cataract Surgery. New England Journal of Medicine, 342(3):168-175.
Publisher | Google Scholor - Mahmood, S. R., Lobo, S. A., Fischer, S. (2023). Cardiac Risk Assessment. In StatPearls [Internet]. StatPearls Publishing.
Publisher | Google Scholor - Thompson, A., Fleischmann, K. E., Smilowitz, N. R., de Las Fuentes, L., Mukherjee, et al. (2024). 2024 AHA/ACC/ACS/ASNC/HRS/SCA/SCCT/SCMR/SVM Guideline for Perioperative Cardiovascular Management for Noncardiac Surgery: A Report of The American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Journal of The American College of Cardiology, 84(19):1869-1969.
Publisher | Google Scholor - Schiro, A. G., Curtis, D. G. (1988). Asymptomatic Coronary Artery Disease. Heart & Lung: The Journal of Critical Care, 17(2):144-149.
Publisher | Google Scholor - Cohn, P. F., Fox, K. M., Daly, C. (2003). Silent Myocardial Ischemia. Circulation, 108(10):1263-1277.
Publisher | Google Scholor - Shams, P., Gul, Z., Makaryus, A. N. (2024). Silent Myocardial Ischemia. In StatPearls [Internet]. StatPearls Publishing.
Publisher | Google Scholor - Bangalore, S., Bates, E. R., Beckie, T. M., Bischoff, J. M., Bittl, J. A., et al. J. (2022). 2021 ACC/AHA/SCAT Guideline for Coronary Artery Revascularization. Journal of The American College of Cardiology, 79(2):E21-E129.
Publisher | Google Scholor























