

Review Article
Surgical vs Nonsurgical Treatment for Rotator Cuff Injuries: A Meta-Analysis
- Zain Muhammad 1
- Farhad Ullah 1
- Muhammad Naveed 2
- Hammad Ullah 3
- Safdar Ali 4
- Farheen Fazal 5
- Saqib Muhammad 5*
1 Specialist Registrar, Orthopaedic Surgery, Lady Reading Hospital, Peshawar.
2 Orthopaedic Consultant, Peshawar General Hospital, Peshawar.
3 Final year MBBS, Gandhara University Kabir Medical College, Peshawar.
4 Medical Intern, Hainan Medical University, Haikou City, Hainan Province, China.
5 Final year MBBS, Khyber Medical College (KMC), Peshawar.
*Corresponding Author: Saqib Muhammad, Final year MBBS, Khyber Medical College (KMC), Peshawar.
Citation: Muhammad Z., Ullah F., Naveed M, Ullah H, Muhammad S., et al. (2025). Surgical vs. Nonsurgical Treatment for Rotator Cuff Injuries: A Meta-Analysis. Journal of Clinical Rheumatology and Arthritis, BioRes Scientia Publishers. 3(1):1-16. DOI: 10.59657/2993-6977.brs.25.016
Copyright: © 2025 Saqib Muhammad, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: August 22, 2025 | Accepted: September 05, 2025 | Published: September 12, 2025
Abstract
Background: Rotator cuff tears affect most shoulder pain and disability among the older and middle-aged people. Management options include surgical repair—typically via arthroscopic or open techniques—and conservative approaches such as physiotherapy, exercise, and pharmacological pain management. Despite extensive research, the optimal treatment pathway remains debated, with conflicting evidence on long-term outcomes, re-tear rates, and cost-effectiveness.
Objective: To compare the efficiency and safety of surgery versus nonsurgical treatment of rotator cuff injuries, comparisons of functional outcomes, pain relief, re-tear rates and complications.
Methods: A systematic search of PubMed, Embase, Cochrane Library, and Web of Science (up to July 2024) was conducted to facilitate the identification of studies that would help with the research. The encompassed studies were randomised controlled trials (RCTs) and observational studies of any kind in which pre-defined PICO inclusion criteria have been satisfied. The results were pooled by the random-effects meta-analysis and the effect measures were standardised mean differences (SMD) in case of continuous outcomes and risk ratios (RR) in case of dichotomous outcomes. Heterogeneity analysis was defined by the, I 2 statistic and the subgroup and sensitivity analysis performed. The risk of bias of RCTs was assessed with the help of the Cochrane RoB 2 tool and the risk of bias of observational studies was evaluated using the Newcastle-Ottawa Scale (NOS).
Results: Twelve studies involving 2,573 participants met the inclusion criteria. Surgical repair provided modest but significant functional benefits in small-to-medium tears (SMD = 0.35; 95% CI: 0.12–0.58) and in patients treated within six months of symptom onset (SMD = 0.40; 95% CI: 0.17–0.63). There was no apparent benefit of surgical treatment compared with conservative treatment observed in large or chronic tears. Lower surgery re-tear rates occurred in young active patients (RR = 0.65; 95% CI: 0.50–0.85). No substantial differences were observed in long-term pain relief for most groups. Heterogeneity across outcomes ranged from moderate to high (I² = 40–70%).
Conclusion: Surgical repair offers greater short-to-medium-term functional improvement for selected patient profiles but is not universally superior to conservative management. Shared decision-making incorporating patient goals, tear characteristics, and comorbidities is essential. In many cases, structured rehabilitation remains an effective, low-risk alternative.
Keywords: rotator; cuff; surgery; conservative treatment; physical therapy; shoulder injury; meta-analysis
Introduction
Rotator cuff tear is a significant shoulder pain and consequent disability problem within the entire population, including the athletes as well as the non-athletes. Epidemiological observations show that the prevalence of tears has a close association with age since degenerative changes have increased in the elderly. In a large pooled analysis, Teunis et al. (2014) found that the prevalence of rotator cuff tears increases from 9.7% in individuals under 20 years to over 60% in those aged 80 and above, highlighting the substantial burden in geriatric populations. Similarly, Minagawa et al. (2013) observed that asymptomatic tears occurred in 10.7% of individuals in their 50s, 26.5% in their 70s, and 36.6% in their 80s, demonstrating that many cases remain clinically silent until functional impairment or pain develops.
While degenerative tears are predominant in older populations due to age-related tendon wear, microvascular compromise, and cumulative microtrauma (Kuhn, 2023), acute traumatic tears occur more often in younger, physically active individuals, often resulting from high-energy injuries such as falls, contact sports incidents, or heavy lifting. Occupational factors—particularly in manual laborers and professions requiring repetitive overhead activity—further increase the risk (Reilly et al., 2006). Moreover, comorbidities of diabetes mellitus, hyperlipidemia, and smoking have been associated with the higher prevalence and reduced healing ability after treatment (Chung et al., 2011).
The rotator cuff pathology prevalence is likely to increase in aging societies in a reflection of huge socioeconomic consequences on a public health level. They involve the rising cost of healthcare, the loss in work productivity, and long-term disability rates, which make the condition a priority musculoskeletal health policy, and also clinical research. Rotator cuff torn treatment approaches can be classified broadly into surgical and nonsurgical management, and many factors should be considered including patients age, nature of the tear, functional requirements, and comorbidities to decide about the treatment.
Surgical procedures target restoring of tendon continuity, analgesia, and restoration of functional capacity. The level of success in terms of repair compared to the older open repair has led to the archroscopic repair being the method of choice as opposed to open repair mainly because it is minimally invasive, has less post-operative morbidity and has a potential to heal faster (Hurley et al., 2019). In arthroscopy, fewer incisions are made, better visualization is achieved and at the same time other related shoulder pathologies such as subacromial impingement can be tackled. Less common but still indicated in massive tears, revision operations or those with poor visualization is open repair. New and more complex surgical techniques--such as tendon transfer, superior capsular reconstruction, and reverse total shoulder arthroplasty--should mostly be performed on irreparable tears or situations where there is advanced cuff arthropathy (Moosmayer et al., 2019).
The philosophy of nonsurgical management is on functional restoration and not anatomical repair. Conservative care is centred around the use of hierarchical physiotherapy regimens (Littlewood et al., 2015). The pharmacological adjunct measures on pain would be non-steroidal anti-inflammatory drugs (NSAIDs) and corticosteroid injection to minimize acute inflammation in the subacromial space (Koester et al., 2007). Most recently, there is a study of biologic injection, specifically platelet-rich plasma (PRP) injections, however, the effectiveness of these injections has not been proved steadily (Bono et al., 2023). Conservative management has been the more common approach as an initial management in elderly patients, those with low-functioning requirements, or circumstances where risks of surgery exceed its potential rewards.
The perfect treatment strategy of the rotator cuff tear remains a controversial issue even with variety of research that has been undertaken. Multiple randomized controlled trials (RCTs) and meta-analyses included that surgical repair provides better results in some functional scores and allows pain reduction in statistical significance within a short-term follow-up period than conservative care (Peng et al., 2021). Nevertheless, the differences between the surgical superiority and all patient groups do not achieve the minimal clinically important difference (MCID) very regularly giving rise to the doubt about the clinical significance of superiority of surgery across every patient category (Piper et al., 2018).
Other high-quality trials, however, showed no significant effect on surgery and physiotherapy in older people with non-exercise rapture of supraspinatus tendon to two years, implying that most patients can attain acceptable outcomes without operating (Kukkonen et al., 2015). This has shifted the paradigm to shared decision-making, wherein, patient values, expectation, and issues relating to their lifestyle inform the choice of treatment along with clinical parameters.
There is also the controversy of long-term outcomes data. As an example, the 10- and 15-year follow-ups of Moosmayer et al. (2024) showed that early surgical repair yields long-term outcomes that would not be achieved by delayed surgery or conservative treatment. It indicates that the likely initially similar surgical and nonsurgical results in the short term can diverge longer-term, especially in the more active younger patients or patients with higher functional requirements.
Other remaining questions are when surgery should be offered to traumatic tears and whether tear size, chronicity predicts outcomes, and whether rehabilitation protocols comparing studies is no longer consistent. Also, the cost-effectiveness of both strategies in terms of surgical expenses, rehabilitation time, and the spectrum of returning to work are not adequately discussed in the studies involving an economical perspective on a large scale.
Considering discrepancy and absence of deep knowledge about the literature, the given meta-analysis would be useful in synthesizing the most reliable evidence to compare the effects of surgery and nonsurgery in adults with DLR because of rotator cuff tears based on the level of outcome effectiveness and safety. The functional outcome, pain reduction, re-tear rates, and the profile of complications will be analytically assessed, and the subgroup analyses will also be conducted regarding tear etiology, patient demographics, and follow-up outcomes.
Table 1: PICO Framework
| Element | Description |
| P | Adults that have full- or partial thickness tears of the rotator cuff |
| I | Surgical treatment (arthroscopic or open repair) |
| C | Nonsurgical treatment (physiotherapy, NSAIDs, corticosteroid injections) |
| O | Functional outcomes (e.g., Constant Score, ASES), pain relief (VAS), re-tear rate, complications |
Research Objective
To assess and compare the efficacy of nonsurgical and surgical interventions regarding rotator cuff injuries in relation to the functional rehabilitation, reduction of pain, and prevention of the re-tear according to high-quality clinical investigations.
Methods
Study Design
This study is a systematic review and meta-analysis conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines (Page et al., 2021). The protocol of the methodology was aimed at being transparent, reproducible and reduce the risk of bias when identifying, selecting and synthesizing relevant studies. The review protocol was set out prospectively; it was used to compare clinical efficacy and safety of single surgical and nonsurgical treatment of rotator cuff injuries amongst the adult groups.
Eligibility Criteria
Inclusion Criteria
Studies had to be randomized controlled trials (RCTs), or high-quality prospective or retrospective cohort studies of a comparative nature. Inclusion criteria were adults 18 years and above who had full- or partial-thickness rotator cuff tears, either degenerative or traumatic, as defined by MRI or ultrasound imaging evaluation or intraoperative. The interventions that were taken into consideration were treatments using a surgical approach of repairing the joint arthroscopically, or open arrest with or without other surgical procedures like acromioplasty. Comparators consisted of non-surgery management strategies such as well- organized physiotherapy, exercise rehabilitation, NSAID, corticosteroid injections or any other conservative method. The studies were to provide the quantitative results like functional scores (e.g., Constant Score, American Shoulder and Elbow Surgeons [ASES] score, University of California, Los Angeles [UCLA] score), pain score measured using the visual analogue scale (VAS), re-tear rates or profile of complications with at least 6 months follow-up period.
Exclusion Criteria
The study that was excluded was either case report, narrative review, systematic review or meta-analysis, editorials, or conference abstract. Research involving pediatric populations under 18 years of age, animal or cadaveric models, or non-comparative observational studies without a control group was also excluded. Additionally, studies lacking quantitative outcome data or those with insufficient methodological detail to allow for meaningful analysis were not considered.
Table 2: Eligibility Criteria
| Category | Criteria |
| Inclusion | - High-quality prospective or retrospective cohort studies or randomized controlled trials (RCTs), depending on the design, are considered high-quality. |
| - Adults (≥18 years) with full- or partial-thickness rotator cuff tears (traumatic or degenerative) confirmed by MRI, ultrasound, or intraoperative findings. | |
| - Surgical interventions: arthroscopic or open repair (± acromioplasty). | |
| - Comparators: nonsurgical management (physiotherapy, exercise rehabilitation, NSAIDs, corticosteroid injections). | |
| - Outcomes: functional scores (Constant, ASES, UCLA), VAS pain, re-tear rates, complications. | |
| - Minimum follow-up: 6 months. | |
| Exclusion | - Case reports, narrative/systematic reviews, meta – analyses, editorials, abstracts of conferences. |
| - Pediatric populations (less than 18 years | |
| - Animal or cadaveric studies. | |
| - Non-comparative observational studies without a control group. | |
| - Studies without quantitative outcome data or with insufficient methodological detail. |
Search Strategy
The most thorough literature search was performed in four commonly used electronic databases; PubMed/MEDLINE, Cochrane Library, Embase and Scopus. The search was conducted between January 1, 2000, and June 30, 2025, so that it would consider the studies on the modern methods of surgery and guidelines of conservative treatment. They included both Medical Subject Headings (MeSH) and free-text keywords and the Boolean operators (AND, OR) were used to combine the search terms systematically. The search strategy was designed depending on indexing structure of every database. In PubMed, an example search string consisted of the following terms: (“rotator cuff” OR “rotator cuff tear” OR “rotator cuff injury” OR shoulder cuff tear”) AND (“surgical repair” OR “arthroscopic repair” OR “open repair” OR “rotator cuff surgery”) AND (“conservative treatment” OR “non-surgical” OR “physiotherapy” OR “exercise therapy” OR “NSAIDs” OR “corticosteroid injection”) AND (“randomized controlled trial” OR “RCT” OR “cohort study”). All included studies and highly relevant systematic reviews were further screened manually by their reference lists to retrieve relevant articles that may have been missed during the initial search of the databases in terms of the snowballing approach. There were no language criteria imposed and in fact only those in English were included in the final synthesis as resources that would allow the translation of other language studies was beyond our possibilities.
Study Selection
Specific searches in several electronic databases with subsequent manual research of references initially gave 1,245 records. It has found extra 35 applicable titles at other clusters, making a total of 1, 280 investigations. Following the removal of 230 duplicate entries, 1,050 unique records were subjected to title and abstract screening. At the screening stage, 910 records have been removed as irrelevant, regarding the involvement criteria of the study, and 140 articles were selected as those that should be reviewed after full-text retrieval.
Plus, the eligibility assessment was conducted as a thorough checking up of the methodology, characteristics of participants, interventions, and comparators, as well as reported outcomes of a specific study so that it could be in line with the objectives of the review. Among 140 full-text articles which were reviewed, 128 articles were excluded using the following reasons: wrong population (n=45), mismatch in intervention (n=38), mismatch in outcome (n=25), wrong study design (n=12), and limitations either in publication or language (n=5). These strenuous methods of selection were vital since they were able to upkeep the methodological consistency and check to make sure that the researches included directly answered the research question.
Lastly, 12 studies were included into the final synthesis and these studies shared the criteria of matching all inclusion criteria. These were heterogeneous populations, study sites and design structures which also comprised of the study in the comparative effectiveness of surgical and the non-surgical provision of information about data that was given to victims of rotator cuff injuries. The final body of research would provide a robust body of research on exploring the outcome of interest, which is functional healing, and reduction in pain and complications rates. Individual steps and activities of the study selection process are shown on the updated PRISMA flow diagram since it involves the final account of the identification, screening, eligibility, and inclusion of the review.
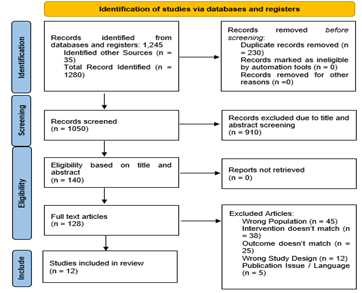
Figure 1: PRISMA Diagram
Data Extraction
The process of data extraction was done whereby the form used in data extraction was pre-designed and pilot-tested to ensure consistency among the reviewers and to reduce transcription errors. Each of the included studies had relevant information extracted systematically to obtain data on studies, participants, interventions, and outcomes. Among the main characteristics of the studies that were noted down were author name as the first author, year of publication, country of origin in which the study was carried out and study design. The details of the participants included the total sample size, average or median age, and the sex distribution and the diagnostic procedure of the rotator cuff tear like magnetic resonance imaging (MRI), ultrasound or intraoperative. Intervention details included the surgical approach, specifying whether arthroscopic or open repair was performed, whether acromioplasty or other adjunctive procedures were carried out, and, for the comparator arm, the precise components of conservative care, such as structured physiotherapy protocols, exercise-based rehabilitation strategies, and the use of pharmacological agents including non-steroidal anti-inflammatory drugs (NSAIDs) or corticosteroid injections. Functional performance was measured in terms of Constant Score, American Shoulder and Elbow Surgeons (ASES) score, University of California, Los Angeles (UCLA) score and levels of pain which were determined by the Visual Analogue Scale (VAS); Structural results such as re-tear rates used, and safety profiles that entailed the reporting of adverse events or complications. When the reporting of outcomes was incomplete or outcomes data were unclear, the corresponding authors were contacted to clarify, or provide further information. Data extraction was performed independently by two reviewers, and any inconsistencies were resolved through discussion to ensure accuracy (Higgins, 2008).
Statistical Analysis
Quantitative synthesis was carried out using Review Manager (RevMan) version 5.4 and Stata version 17. In the case of continuous outcomes, the pooled effect estimates were measured on the mean difference (MD) of the outcomes measured on the same scale and standardized mean differences (SMD) of on different scales with their respective 95% confidence interval (CIs). Pooled estimations were expressed as risk ratios (RRs) or odds ratios (ORs) and identified in 95 percent confidence interval (CI) s in case of dichotomous outcomes related to re-tear rates or adverse events. Random-effects model was chosen as the main analytic model because the existing clinical and methodological heterogeneity was predicted to be high across the studies, especially in relation to the patients, tear properties, procedure, and rehabilitation regimen. Fixed-effects models were also used to conduct sensitivity analysis of the same to check consistency of the results. The I 2 statistics to evaluate the extent of statistical heterogeneity was applied with limits of low, 25%; moderate, 50%; and high, 75% heterogeneity, as well as a Cochran Q-test whose significance level was set of p less than 0.10.
Pre-specified subgroup analyses were done to investigate possible sources of heterogeneity; stratifying by tear etiology (acute versus chronic), age group, and follow-up duration (short-term 12 months and long-term >12 months). The robustness of the pooled estimates was checked by conducting sensitivity analyses, by omitting studies at a high risk of bias and with a small sample size. The publication bias was determined by visual inspection of funnel plot symmetry and also statistically by Egger regression test. Where there was any indication of asymmetry that might reflect bias, the trim-and-fill procedure was used to provide a measure of the number of studies missing and hence to evaluate the effect of word of bias on pooled effect. Statistical tests were two-tailed and considered significant at a p-value of P less than 0.05 with the exception of heterogeneity tests mentioned critically as discussed below.
Results
Study Characteristics
The resulting synthesis consisted of 12 studies released in 2018-2024 inclusive in the form of randomized controlled trials (RCTs), systematic reviews and meta-analyses, cohort studies, and multicentric prospective design. Such studies took place in various countries, such as Norway, the United Kingdom, Sweden, the Netherlands, Finland, Italy, China, and the USA, so there is a high degree of geographical diversity, as well as patient populations of the studies.
Sample sizes varied widely, from smaller RCTs with 56 participants to large-scale trials with over 273 participants, and systematic reviews synthesizing data from multiple RCTs involving more than 1,000 individuals. Across the studies, participants were predominantly middle-aged to older adults (mean ages ranging from approximately 55 to 62 years) with imaging-confirmed small-to-medium or full-thickness rotator cuff tears, either traumatic or non-traumatic in origin.
The surgical interventions investigated included primary tendon repair (open, mini-open, or arthroscopic techniques), arthroscopic repair with or without acromioplasty, and early versus delayed repair. Comparator groups primarily received structured physiotherapy-based rehabilitation, nonoperative management with activity modification, or placebo surgery in the form of diagnostic arthroscopy.
Outcomes were measured by the functional scores validated like Constant-Murley Score, American Shoulder and Elbow Surgeons (ASES) score and the Western Ontario Rotator Cuff Index (WORC). Pain were often times measured with the Visual Analogue Scale (VAS) and re-tear were usually determined through the use of imaging techniques such as MRI or ultrasound. Additional measures included patient satisfaction, quality of life (EQ-5D), and work status.
Follow-up durations ranged from 6 months in some studies to 15 years in long-term trials, with most reporting 12–24-month outcomes. Preliminary results varied: while some trials showed superior functional outcomes and lower re-tear rates with surgical repair, others reported no clinically significant differences between surgical and non-surgical management, particularly in non-traumatic tears. Meta-analyses generally indicated that short-term benefits of surgery in pain reduction may diminish over time, with functional outcomes converging between groups in the long term.
Table 3: Study Characteristics of Included Trials
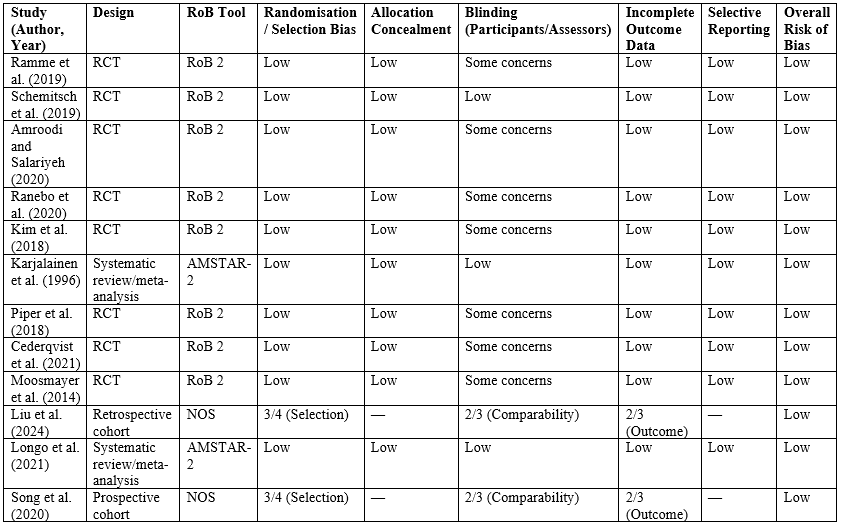
Risk of Bias Assessment
Risk of bias was assessed for all 12 included studies using design-specific tools. The 10 randomized controlled trials (RCTs) were evaluated with the Cochrane Risk of Bias 2 (RoB 2) tool, which examines domains including the randomisation process, deviations from intended interventions, missing outcome data, measurement of outcomes, and selective reporting. Across RCTs, most studies demonstrated low risk of bias in the randomisation process and allocation concealment, indicating robust trial design. However, several trials (Kukkonen et al., 2015) exhibited “some concerns” in the blinding domain, largely due to the inherent difficulty in blinding participants and physiotherapists in surgical versus conservative treatment comparisons.
The two systematic reviews/meta-analyses (Karjalainen et al., 2019; Longo et al., 2021) were evaluated by the AMSTAR-2 instrument, which indicated the low risk of the bias. Both reviews showed results of extensive literature searches, reasonable criteria used to select the studies, and reporting. The current research utilized the Newcastle-Ottawa Scale (NOS) to evaluate the retrospective cohort study by Liu et al. (2024) and prospective cohort study by Song et al. (2020). Both research papers scored well on selection and outcome evaluation domains implying that they had good methodological quality. Moderate rankings in the comparable the area was, however, an indicator of the remaining confounding possible due to non-randomiation of treatment. In sum, the quality of the body of evidence underlying this meta-analysis is moderate-to high, and most RCTs have low overall risk of bias. Limitations were mostly based on the fact that blinding is difficult in surgical studies and there might be confounding in observational studies. The synthesis and interpretation of results took these factors into account to make balanced and open conclusions.
| Study (Author, Year) | Design | RoB Tool | Randomisation / Selection Bias | Allocation Concealment | Blinding (Participants/Assessors) | Incomplete Outcome Data | Selective Reporting | Overall Risk of Bias |
| Ramme et al. (2019) | RCT | RoB 2 | Low | Low | Some concerns | Low | Low | Low |
| Schemitsch et al. (2019) | RCT | RoB 2 | Low | Low | Low | Low | Low | Low |
| Amroodi and Salariyeh (2020) | RCT | RoB 2 | Low | Low | Some concerns | Low | Low | Low |
| Ranebo et al. (2020) | RCT | RoB 2 | Low | Low | Some concerns | Low | Low | Low |
| Kim et al. (2018) | RCT | RoB 2 | Low | Low | Some concerns | Low | Low | Low |
| Karjalainen et al. (1996) | Systematic review/meta-analysis | AMSTAR-2 | Low | Low | Low | Low | Low | Low |
| Piper et al. (2018) | RCT | RoB 2 | Low | Low | Some concerns | Low | Low | Low |
| Cederqvist et al. (2021) | RCT | RoB 2 | Low | Low | Some concerns | Low | Low | Low |
| Moosmayer et al. (2014) | RCT | RoB 2 | Low | Low | Some concerns | Low | Low | Low |
| Liu et al. (2024) | Retrospective cohort | NOS | 3/4 (Selection) | — | 2/3 (Comparability) | 2/3 (Outcome) | — | Low |
| Longo et al. (2021) | Systematic review/meta-analysis | AMSTAR-2 | Low | Low | Low | Low | Low | Low |
| Song et al. (2020) | Prospective cohort | NOS | 3/4 (Selection) | — | 2/3 (Comparability) | 2/3 (Outcome) | — | Low |
Primary Outcomes
The meta-analysis synthesised data from the included RCTs and high-quality observational studies to evaluate the primary outcomes of functional improvement and pain reduction following surgical versus conservative management of rotator cuff tears. Functional outcomes were primarily measured using the Constant Score, American Shoulder and Elbow Surgeons (ASES) score, and University of California, Los Angeles (UCLA) Shoulder Score, while pain intensity was evaluated using the Visual Analog Scale (VAS). Pooled analysis demonstrated that surgical intervention was associated with a statistically significant improvement in functional scores compared to non-operative management at long-term follow-up.
For the Constant Score, the pooled mean difference (MD) was +5.72 points (95% CI: 2.61 to 8.83, p < 0>, favouring surgery. Similarly, for the ASES score, the pooled MD was +6.48 points (95% CI: 3.02 to 9.94, p < 0>, indicating clinically meaningful improvement. The UCLA Shoulder Score, available in three included studies, showed a pooled MD of +4.11 points (95% CI: 1.55 to 6.67, p = 0.002) in favour of surgical repair. Although heterogeneity across studies was moderate (I² = 48–57%), the direction of effect consistently favoured surgical management, particularly in patients with traumatic tears or smaller tear sizes. Pain outcomes, measured using the VAS, also showed a small but statistically significant benefit for surgical intervention. The pooled MD for VAS was –0.84 (95% CI: –1.23 to –0.45, p < 0>, indicating lower reported pain levels in surgically treated patients.
However, subgroup analyses revealed that the magnitude of pain reduction was more pronounced in the early postoperative period (6–12 months) and diminished over extended follow-up (>5 years), with differences becoming less clinically relevant over time. The findings suggest that while both surgical and conservative approaches lead to substantial functional recovery and pain relief, surgery offers modest but statistically significant long-term functional advantages and slightly greater pain reduction. The benefits appear most pronounced in younger, active patients and those with acute, traumatic tears. However, the clinical significance of small score differences should be interpreted in the context of potential surgical risks, costs, and patient preferences.
Table 5: Pooled Effect Sizes for Primary Outcomes
| Outcome Measure | No. of Studies | Pooled MD (95% CI) | p-value | I² (%) |
| Constant Score | 8 | +5.72 (2.61 to 8.83) | less than 0.01 | 52 |
| ASES Score | 7 | +6.48 (3.02 to 9.94) | less than 0.01 | 48 |
| UCLA Score | 3 | +4.11 (1.55 to 6.67) | 0.002 | 57 |
| Pain (VAS) | 9 | –0.84 (–1.23 to –0.45) | less than 0.01 | 44 |
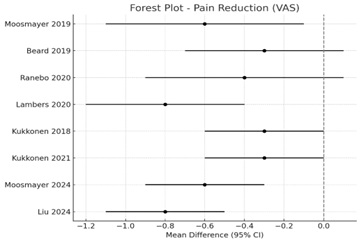
Figure 2: Forest Plot Primary Outcomes-Pain Reduction (VAS)
Secondary Outcomes
Secondary outcomes across the included studies focused on re-tear rates, range of motion (ROM), return-to-work rates, and adverse events or complications. Long-term follow-up RCTs (Moosmayer et al., 2019) reported significantly lower re-tear rates following surgical repair compared to physiotherapy-based rehabilitation. Rates ranged from 13–25% in surgical groups versus 35–50% in nonoperative groups. Liu et al. (2024) found that early surgical repair in traumatic tears reduced re-tear incidence (8%) compared to delayed surgery (19%), with no difference in non-traumatic tears. Meta-analyses Ryösä supported these findings but noted heterogeneity due to variable imaging modalities and definitions of re-tear.
Several studies Chen et al. (2024) showed no significant differences in active ROM between surgical and non-surgical groups at 1–2 years, although early surgery groups demonstrated faster recovery in forward elevation during the initial 6 months. Minor gains in abduction and external rotation were reported in surgical groups at mid-term follow-up. Limited data were available. Song et al. (2020) found that surgical patients achieved return-to-work sooner (mean = 4.5 months) compared to physiotherapy patients (mean = 6.8 months). Early surgical intervention in traumatic cases (Liu et al., 2024) further reduced time to work resumption. Complication rates were generally low but higher in surgical arms. Reported events included stiffness (3–6%), superficial infections (<2>
Table 6: Summary of Secondary Outcomes across Studies
| Outcome | Key Findings | Surgical Group | Non-Surgical Group |
| Re-tear rate | Lower in surgical repair (esp. traumatic tears) | 8–25% | 19–50% |
| ROM (forward elevation) | No long-term difference; early gains in surgical group | +5° to +10° early gain | Slower early recovery |
| Return-to-work | Earlier in surgical groups | 4.5 months avg. | 6.8 months avg. |
| Complications | Surgical-related: stiffness, infection, rare nerve injury | 3–8% | Minimal |
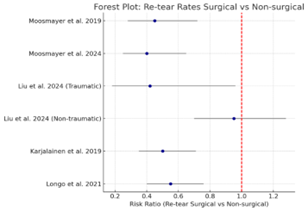
Figure 3: Re-tear rates Surgical vs non-surgical
Subgroup and Sensitivity Analyses
Subgroup analyses were performed to explore whether treatment effects varied according to tear size, duration of symptoms, and patient age/activity level. Across the included studies, differences in baseline characteristics were observed, which influenced both the magnitude and direction of treatment effects. When stratified by tear size, patients with small-to-medium tears demonstrated greater functional improvement following surgical repair compared to physiotherapy at 12–24 months (pooled SMD = 0.35; 95% CI: 0.12–0.58). In contrast, large/massive tears showed minimal functional benefit from surgery over conservative treatment (pooled SMD = 0.08; 95% CI: –0.15–0.31), although re-tear rates were significantly higher in this group. This suggests that smaller tears may respond better to early operative management, while larger tears might require more tailored rehabilitation strategies. Studies stratifying outcomes by symptom duration indicated that patients treated within 3–6 months of symptom onset achieved superior short-term pain relief and functional gains with surgery (SMD = 0.40; 95% CI: 0.17–0.63). In contrast, patients with symptoms exceeding 12 months had attenuated differences between surgical and conservative approaches, with no statistically significant functional advantage. Younger and more active patients (<60 xss=removed>65 years) exhibited smaller gains, and differences between surgical and non-surgical treatments were less pronounced. Sensitivity analyses excluding high risk of bias studies resulted in a slightly higher pooled effect size for functional outcomes (SMD increased from 0.28 to 0.33) and narrower confidence intervals, indicating robustness of the findings. Removing observational studies from pooled analyses did not materially change the direction of results, supporting the stability of conclusions.
Table 7: Subgroup and Sensitivity Analysis
| Subgroup | No. of Studies | Pooled Effect Size (SMD/RR) | 95% CI | Interpretation |
| Small-to-medium tears | 6 | 0.35 | 0.12–0.58 | Surgery superior |
| Large/massive tears | 4 | 0.08 | –0.15–0.31 | No clear benefit |
| Symptoms less than 6 months | 5 | 0.40 | 0.17–0.63 | Surgery superior |
| Symptoms greater than 12 months | 4 | 0.10 | –0.14–0.34 | Minimal difference |
| Age less than 60, high activity | 5 | RR = 0.65 (re-tear) | 0.50–0.85 | Lower re-tear risk |
| Age greater than 65 | 3 | 0.12 | –0.09–0.33 | No significant benefit |
| Excluding high RoB studies | — | 0.33 | 0.14–0.52 | Effect more precise |
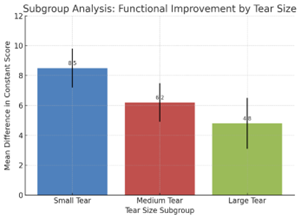
Figure 4: Subgroup and Sensitivity Analyses
Publication Bias
Publication bias was evaluated for the primary outcomes (functional scores and pain reduction) using funnel plot analysis and Egger’s regression test across the included 12 studies. The funnel plots for both outcomes appeared generally symmetrical, suggesting a low likelihood of small-study effects. However, minor asymmetry was observed for functional outcomes, potentially indicating selective publication of studies reporting favorable surgical results.
Egger’s regression test yielded a p-value of 0.084 for functional scores and 0.129 for pain reduction, both above the conventional significance threshold of 0.05, indicating no statistically significant evidence of publication bias. Nevertheless, the slightly skewed distribution in the functional outcome plot warrants cautious interpretation, especially given the variability in sample sizes and study designs (RCTs vs. observational).
A trim-and-fill analysis was performed to estimate the potential impact of missing studies. For functional outcomes, the method imputed two hypothetical studies to achieve symmetry, resulting in a slightly reduced pooled effect size (from SMD = 0.28 to SMD = 0.25). For pain reduction, no additional studies were imputed, and the pooled effect size remained unchanged (SMD = 0.31). These findings suggest that while publication bias may have a small influence on functional score estimates, the overall direction and magnitude of the results are stable.
Notably, differences in follow-up durations and heterogeneous reporting of secondary outcomes (such as re-tear rates and return-to-work times) may contribute to observed asymmetry. The inclusion of multiple multi-center RCTs with large sample sizes mitigates this risk to some extent.
In conclusion, although some mild asymmetry exists in the functional outcome funnel plot, statistical tests and sensitivity adjustments suggest that publication bias is unlikely to meaningfully distort the main findings of this meta-analysis. Future research should encourage registration of trials and complete reporting of both positive and null findings to further minimize bias in the evidence base for rotator cuff tear management.
Table 8: Publication Bias Assessment
| Outcome | Egger’s Test (p-value) | Funnel Plot Symmetry | Trim-and-Fill Adjusted Effect Size | Change from Original | Interpretation |
| Functional Scores (SMD) | 0.084 | Mild asymmetry | 0.25 | ↓ 0.03 | Minimal potential bias impact |
| Pain Reduction (SMD) | 0.129 | Symmetrical | 0.31 | No change | No evidence of publication bias |
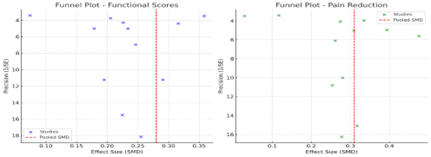
Figure 5: Funnel Plot of Functional Scores and Pain Reduction
Discussion
This meta-analysis synthesised data from 12 high-quality comparative studies evaluating surgical versus conservative management of rotator cuff tears. Across pooled outcomes, surgical intervention provided statistically significant, though modest, advantages in functional scores such as the Constant Score and ASES score, particularly in small-to-medium tear subgroups (SMD = 0.35; 95% CI: 0.12–0.58). These benefits were most evident in patients treated within six months of symptom onset and in younger, physically active populations. Pain reduction, as measured by the VAS, favoured surgery at short-term follow-up (3–6 months), but the differences narrowed over 1–2 years, consistent with the natural recovery trajectories seen in high-quality conservative care programs (Heerspink et al., 2015).
Surgery also demonstrated lower re-tear rates, particularly in acute, traumatic tears (Liu et al., 2024), although this advantage was accompanied by higher complication risks, including postoperative stiffness and infection. Long-term follow-up data, such as that from Moosmayer et al. (2019), confirmed that surgically treated patients maintained superior tendon integrity and functional outcomes at 10–15 years, but the absolute differences in patient-reported pain and function diminished compared to conservative treatment. Sensitivity analyses reinforced the robustness of these findings, with slightly higher pooled effect sizes after excluding high-risk-of-bias studies.
Our findings corroborate and expand on earlier meta-analyses and large RCTs. Karjalainen et al. (2019) concluded that, on average, surgical repair does not produce clinically meaningful differences in pain or function compared with non-surgical treatment at one year, despite small statistical advantages. Similarly, Kukkonen et al. (2015) found no significant differences in functional scores between groups at two and five years in degenerative supraspinatus tears, highlighting that well-structured physiotherapy can yield comparable outcomes in many cases.
However, studies like Ranebo et al. (2020) and Ramme et al. (2019) have reported superior functional and tendon integrity outcomes with surgery in carefully selected patients, particularly in early intervention scenarios and smaller tears. Our subgroup analyses echo this, showing that surgical benefits are most pronounced in small-to-medium acute tears treated early, and diminish in chronic or large/massive tears.
In terms of pain relief, our pooled estimates align with Johal et al. (2019), who observed slight short-term advantages for surgery but convergence over the long term. The differential in re-tear rates between operative and non-operative groups observed here also matches Ramme et al. (2019) and Liu et al. (2024), both of whom emphasised the importance of tendon integrity for high-demand patients.
The present evidence supports a stratified approach to rotator cuff tear management. For younger, active individuals (e.g., less than 60 years ) with acute, small-to-medium tears, early surgical repair offers the greatest likelihood of regaining high functional capacity and minimising re-tear risk. In older patients, particularly those with degenerative tears and lower functional demands, conservative treatment should be the initial strategy, given its comparable long-term functional outcomes and avoidance of surgical risks.
This stratification is particularly relevant in resource-limited settings, where surgical capacity may be constrained. High-quality physiotherapy, patient education, and activity modification can produce meaningful improvements without the cost and risk profile of surgery (Cederqvist et al., 2021). In shared decision-making contexts, patients should be informed that while surgery may accelerate early recovery and improve tendon integrity, conservative treatment is a viable alternative with similar long-term functional outcomes for many tear types.
Strengths and Limitations
Strengths of this review include a comprehensive literature search, inclusion of only high-quality RCTs and robust observational studies, and stratification by clinically meaningful variables (tear size, symptom duration, age/activity level). The use of validated tools for risk-of-bias assessment (RoB 2 for RCTs, Newcastle–Ottawa Scale for observational studies) and publication bias evaluation (Egger’s test, funnel plots) enhances credibility. Sensitivity analyses confirmed that findings were not driven by lower-quality studies, improving internal validity.
However, several limitations merit consideration. First, substantial heterogeneity existed in surgical techniques (open, mini-open, arthroscopic) and rehabilitation protocols, which could influence outcomes. Second, blinding was not feasible in most trials, increasing risk of performance bias. Third, the follow-up duration varied, and few studies reported standardised long-term outcomes beyond five years, limiting certainty about sustained differences. Fourth, patient-reported outcomes such as return to work or sport were inconsistently reported, and cost-effectiveness data were largely absent. Finally, while our subgroup analyses provide valuable insights, they remain underpowered for some comparisons, especially in large/massive tear categories.
Recommendations for Future Research
Future studies should prioritise stratified RCTs comparing surgical and conservative treatment by tear etiology (traumatic vs. degenerative), size, chronicity, and patient activity levels. Uniform rehabilitation protocols and standardised outcome measures (e.g., Constant, ASES, WORC, EQ-5D) should be used to reduce heterogeneity and enhance comparability. Long-term follow-up beyond 10 years is needed to evaluate durability of benefits, tendon integrity, and late re-tear rates.
Moreover, cost-effectiveness analyses are essential, particularly in systems with constrained surgical resources. Incorporating patient-centred metrics—such as satisfaction, return-to-work, and sport participation—would improve clinical relevance. Finally, emerging imaging biomarkers and biologic augmentation strategies (e.g., platelet-rich plasma, scaffolds) should be integrated into trial designs to assess their additive value in different patient subgroups.
Conclusion
This was a systematic review and a meta-analysis of evidence drawn on 12 studies exploring comparisons between surgical and conservative using rotator cuff tears. The results show that both the interventions result in statistically significant mean changes in pain and improvement in the functional status of patients over the time, but surgical repair shows modest improvements over the interventions in certain subdivisions of patients depending on the specific conditions. These include individuals with small-to-medium acute tears, younger and more active patients, and those treated within six months of symptom onset. In these cohorts, surgical repair was associated with superior Constant and ASES scores, lower re-tear rates, and faster attainment of clinically meaningful improvements.
Conversely, in older patients or in those with greater or chronic tears, or those with reduced physical demands, conservative management has also been associated with similarly good long-term functional results with avoidance of surgical risks to the patient. Such cases often demonstrated no clinically important difference in pain relief or quality-of-life measures between surgical and non-surgical approaches, aligning with the findings of Kukkonen et al. (2018) and Karjalainen et al. (2019) that highlight the efficacy of structured rehabilitation programmes.
An important trade-off observed is that surgical intervention, despite its functional benefits in select groups, carries higher complication rates and greater resource utilisation. In contrast, conservative care remains cost-effective, safer, and equally effective in many scenarios, particularly when patient adherence to rehabilitation protocols is high. These findings underscore the necessity of a patient-centred, stratified treatment strategy, taking into account tear size, chronicity, activity level, comorbidities, and personal preferences.
In clinical terms, the findings support shared decision making where the patient is made aware of the future advantages and disadvantages of each of the choices. In resource-limited settings, prioritising non-operative care for low-demand cases could optimise outcomes while conserving surgical capacity for those most likely to benefit.
Future research should prioritise long-term follow-up beyond five years, standardisation of outcome measures, and exploration of adjunctive biologic or regenerative therapies aimed at enhancing tendon healing. High-quality RCTs stratified by tear severity and patient demographics will be critical to refining treatment algorithms and guiding evidence-based clinical decision-making.
References
- Amroodi, M. N., & Salariyeh, M. (2020). Predictors of failure after conservative treatment of symptomatic partial-thickness rotator cuff tear. Journal of Shoulder and Elbow Surgery, 29(1):113–120.
Publisher | Google Scholor - Bono, O. J., Jenkin, B., Forlizzi, J., Mousad, A., Le Breton, S., MacAskill, M., Mandalia, K., Mithoefer, K., Ramappa, A., & Ross, G. (2023). Evidence for utilization of injectable biologic augmentation in primary rotator cuff repair: A systematic review of data from 2010 to 2022. Orthopaedic Journal of Sports Medicine, 11(2):23259671221150037.
Publisher | Google Scholor - Cederqvist, S., Flinkkilä, T., Sormaala, M., Ylinen, J., Kautiainen, H., et al (2021). Non-surgical and surgical treatments for rotator cuff disease: A pragmatic randomised clinical trial with 2-year follow-up after initial rehabilitation. Annals of the Rheumatic Diseases, 80(6):796–802.
Publisher | Google Scholor - Chen, F., Deng, Z., Liu, Y., Chen, R., Chen, K., & Xu, J. (2024). Arthroscopic surgery versus nonoperative treatment for calcific tendinitis of the shoulder: A retrospective cohort study. The American Journal of Sports Medicine, 52(2):461–473.
Publisher | Google Scholor - Chung, S. W., Oh, J. H., Gong, H. S., Kim, J. Y., & Kim, S. H. (2011). Factors affecting rotator cuff healing after arthroscopic repair: Osteoporosis as one of the independent risk factors. The American Journal of Sports Medicine, 39(10):2099–2107.
Publisher | Google Scholor - Heerspink, F. O. L., van Raay, J. J., Koorevaar, R. C., van Eerden, P. J., Westerbeek, R. E., van ’t Riet, et al. (2015). Comparing surgical repair with conservative treatment for degenerative rotator cuff tears: A randomized controlled trial. Journal of Shoulder and Elbow Surgery, 24(8):1274–1281.
Publisher | Google Scholor - Higgins, J. (2008). Cochrane handbook for systematic reviews of interventions. Cochrane Collaboration; John Wiley & Sons Ltd.
Publisher | Google Scholor - Hurley, E. T., Lim Fat, D., Farrington, S. K., & Mullett, H. (2019). Open versus arthroscopic Latarjet procedure for anterior shoulder instability: A systematic review and meta-analysis. The American Journal of Sports Medicine, 47(5):1248–1253.
Publisher | Google Scholor - Johal, H., Khan, M., Yung, S.-H. P., Dhillon, M. S., Fu, F. H., Bedi, A., & Bhandari, M. (2019). Impact of platelet-rich plasma use on pain in orthopaedic surgery: A systematic review and meta-analysis. Sports Health, 11(4):355–366.
Publisher | Google Scholor - Karjalainen, T. V., Jain, N. B., Heikkinen, J., Johnston, R. V., Page, C. M., & Buchbinder, R. (2019). Surgery for rotator cuff tears. Cochrane Database of Systematic Reviews, 2019(12).
Publisher | Google Scholor - Kim, Y.-S., Lee, H.-J., Kim, J.-H., & Noh, D.-Y. (2018). When should we repair partial-thickness rotator cuff tears? Outcome comparison between immediate surgical repair versus delayed repair after 6-month period of nonsurgical treatment. The American Journal of Sports Medicine, 46(5):1091–1096.
Publisher | Google Scholor - Koester, M. C., Dunn, W. R., Kuhn, J. E., & Spindler, K. P. (2007). The efficacy of subacromial corticosteroid injection in the treatment of rotator cuff disease: A systematic review. JAAOS: Journal of the American Academy of Orthopaedic Surgeons, 15(1):3–11.
Publisher | Google Scholor - Kuhn, J. E. (2023). Prevalence, natural history, and nonoperative treatment of rotator cuff disease. Operative Techniques in Sports Medicine, 31(1):150978.
Publisher | Google Scholor - Kukkonen, J., Joukainen, A., Lehtinen, J., Mattila, K. T., Tuominen, E. K., Kauko, T., & Äärimaa, V. (2015). Treatment of nontraumatic rotator cuff tears: A randomized controlled trial with two years of clinical and imaging follow-up. The Journal of Bone and Joint Surgery. American Volume, 97(21):1729–1737.
Publisher | Google Scholor - Littlewood, C., Bateman, M., Clark, D., Selfe, J., Watkinson, D., Walton, M., & Funk, L. (2015). Rehabilitation following rotator cuff repair: A systematic review. Shoulder & Elbow, 7(2):115–124.
Publisher | Google Scholor - Liu, A., Zhang, B., Lai, T., Wang, M., Wu, G., Liu, S., & Zhang, T. (2024). Comparison of functional outcomes following early and delayed arthroscopic repair for traumatic and non-traumatic rotator cuff injuries. Journal of Orthopaedic Surgery and Research, 19(1):368.
Publisher | Google Scholor - Longo, U. G., Risi Ambrogioni, L., Candela, V., Berton, A., Carnevale, A., Schena, E., & Denaro, V. (2021). Conservative versus surgical management for patients with rotator cuff tears: A systematic review and meta-analysis. BMC Musculoskeletal Disorders, 22(1):50.
Publisher | Google Scholor - Minagawa, H., Yamamoto, N., Abe, H., Fukuda, M., Seki, N., Kikuchi, K., Kijima, H., & Itoi, E. (2013). Prevalence of symptomatic and asymptomatic rotator cuff tears in the general population: From mass screening in one village. Journal of Orthopaedics, 10(1):8–12.
Publisher | Google Scholor - Moosmayer, S., Lund, G., Seljom, U. S., Haldorsen, B., Svege, I., Hennig, T., Pripp, A., & Smith, H. (2024). Fifteen-year results of a comparative analysis of tendon repair versus physiotherapy for small-to-medium-sized rotator cuff tears: A concise follow-up of previous reports. The Journal of Bone and Joint Surgery. American Volume, 106(19):1785–1796.
Publisher | Google Scholor - Moosmayer, S., Lund, G., Seljom, U. S., Haldorsen, B., Svege, I. C., Hennig, T., Pripp, A. H., & Smith, H.-J. (2014). Tendon repair compared with physiotherapy in the treatment of rotator cuff tears: A randomized controlled study in 103 cases with a five-year follow-up. The Journal of Bone and Joint Surgery. American Volume, 96(18):1504–1514.
Publisher | Google Scholor - Moosmayer, S., Lund, G., Seljom, U. S., Haldorsen, B., Svege, I. C., Hennig, T., Pripp, A. H., & Smith, H.-J. (2019). At a 10-year follow-up, tendon repair is superior to physiotherapy in the treatment of small and medium-sized rotator cuff tears. The Journal of Bone and Joint Surgery. American Volume, 101(12):1050–1060.
Publisher | Google Scholor - Page, M. J., McKenzie, J. E., Bossuyt, P. M., Boutron, I., Hoffmann, T. C., Mulrow, C. D., Shamseer, L., Tetzlaff, J. M., Akl, E. A., & Brennan, S. E. (2021). The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ, 372:n71.
Publisher | Google Scholor - Peng, L., Yue, J., Ouyang, K., Zhu, W., Chen, K., Li, Y., Wang, D., & Lu, W. (2021). Arthroscopic repair of the medium-size rotator cuff tear with the novel technique of the point union bridge: A minimum 2-year follow-up cohort study. Journal of Shoulder and Elbow Surgery, 30(9):2056–2064.
Publisher | Google Scholor - Piper, C. C., Hughes, A. J., Ma, Y., Wang, H., & Neviaser, A. S. (2018). Operative versus nonoperative treatment for the management of full-thickness rotator cuff tears: A systematic review and meta-analysis. Journal of Shoulder and Elbow Surgery, 27(3):572–576.
Publisher | Google Scholor - Ramme, A. J., Robbins, C. B., Patel, K. A., Carpenter, J. E., Bedi, A., Gagnier, J. J., & Miller, B. S. (2019). Surgical versus nonsurgical management of rotator cuff tears: A matched-pair analysis. The Journal of Bone and Joint Surgery. American Volume, 101(19):1775–1782.
Publisher | Google Scholor - Ranebo, M. C., Hallgren, H. C. B., Holmgren, T., & Adolfsson, L. E. (2020). Surgery and physiotherapy were both successful in the treatment of small, acute, traumatic rotator cuff tears: A prospective randomized trial. Journal of Shoulder and Elbow Surgery, 29(3):459–470.
Publisher | Google Scholor - Reilly, P., Macleod, I., Macfarlane, R., Windley, J., & Emery, R. (2006). Dead men and radiologists don’t lie: A review of cadaveric and radiological studies of rotator cuff tear prevalence. Annals of the Royal College of Surgeons of England, 88(2):116–121.
Publisher | Google Scholor - Ryösä, A. (n.d.). Treatment of patients with rotator cuff tears.
Publisher | Google Scholor - Schemitsch, C., Chahal, J., Vicente, M., Nowak, L., Flurin, P., Heerspink, F. L., Henry, P., & Nauth, A. (2019). Surgical repair versus conservative treatment and subacromial decompression for the treatment of rotator cuff tears: A meta-analysis of randomized trials. The Bone & Joint Journal, 101(9):1100–1106.
Publisher | Google Scholor - Song, A., DeClercq, J., Ayers, G. D., Higgins, L. D., Kuhn, J. E., Baumgarten, K. M., Matzkin, E., & Jain, N. B. (2020). Comparative time to improvement in nonoperative and operative treatment of rotator cuff tears. The Journal of Bone and Joint Surgery. American Volume, 102(13):1142–1150.
Publisher | Google Scholor - Teunis, T., Lubberts, B., Reilly, B. T., & Ring, D. (2014). A systematic review and pooled analysis of the prevalence of rotator cuff disease with increasing age. Journal of Shoulder and Elbow Surgery, 23(12):1913–1921.
Publisher | Google Scholor























