

Case Report
Spleen-Preserving Distal Pancreatectomy for Mucinous Cystic Neoplasm: A Case Report and Review of The Literature
- Houda Ezzaki *
- Karim Ibn Majdoub
- Ahmed Zerhouni
- Tarik Souiki
- Imane Toughrai
General Surgery Department, Centre Hospitalier Universitaire Hassan II, Fes, Morocco.
*Corresponding Author: Houda Ezzaki, General Surgery Department, Centre Hospitalier Universitaire Hassan II, Fès, Morocco.
Citation: Houda Ezzaki, Karim Ibn Majdoub, Ahmed Zerhouni, Tarik Souiki, Imane Toughrai. (2025). Spleen-Preserving Distal Pancreatectomy for Mucinous Cystic Neoplasm: A Case Report and Review of The Literature, International Journal of Clinical and Surgical Pathology, BioRes Scientia Publishers. 2(1):1-3. DOI: 10.59657/3067-0462.brs.25.015
Copyright: © 2025 Houda Ezzaki, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: September 05, 2025 | Accepted: September 16, 2025 | Published: September 19, 2025
Abstract
Background: Background: Mucinous cystic neoplasms (MCN) of the pancreas are rare cystic tumors with malignant potential, typically affecting middle-aged women and predominantly located in the pancreatic body and tail. Surgical resection remains the treatment of choice.
Case Presentation: We report the case of a 50-year-old woman presenting with vague abdominal pain. Imaging revealed a well-defined, round cystic lesion in the pancreatic tail with calcifications. A spleen-preserving distal pancreatectomy was performed with an uneventful postoperative course. Histopathological analysis confirmed a mucinous cystic neoplasm without invasive features.
Discussion: Spleen preservation during distal pancreatectomy reduces the long-term risk of overwhelming post-splenectomy infection (OPSI), a rare but potentially fatal complication. Several studies have demonstrated decreased postoperative morbidity with spleen-preserving approaches, albeit at the cost of longer operative times. Preservation of the splenic vessels reduces the risk of splenic infarction compared with vessel resection.
Conclusion: Spleen-preserving distal pancreatectomy is a safe and effective surgical option for MCN, allowing preservation of immunological function while achieving oncological safety.
Keywords: spleen-preserving distal pancreatectomy; mucinous cystic neoplasms; overwhelming post-splenectomy infection
Introduction
Mucinous cystic neoplasms (MCN) of the pancreas are uncommon cystic tumors with potential for malignant transformation into cystadenocarcinoma. They predominantly affect women in their 4th to 5th decade of life, with 70-90% located in the body or tail of the pancreas. Given their premalignant nature, surgical resection is generally recommended. Distal pancreatectomy with or without splenectomy is the standard procedure. However, spleen preservation is increasingly advocated to reduce postoperative infectious risks and maintain long-term immunological function.
Case Report
A 50-year-old woman, with no significant past medical history, presented with vague abdominal pain lasting for 6 months. Abdominal ultrasound revealed a unilocular cystic lesion with thick walls. Contrast-enhanced CT scan demonstrated a well-defined hypodense lesion in the pancreatic tail, measuring 15×18 mm, with peripheral calcifications. The patient underwent a distal pancreatectomy with spleen preservation using splenic vessel conservation. The postoperative course was uneventful. Final histopathology confirmed a mucinous cystic neoplasm without invasive features.
Discussion
Mucinous cystic neoplasms (MCN) are premalignant lesions that require surgical excision in most cases due to their potential progression to invasive carcinoma. Their epidemiological profile-predominantly affecting women, with a mean age of 40-50 years and a predilection for the pancreatic body and tail-is well documented. In the present case, the clinical, radiological, and pathological features were consistent with typical MCN.
Rationale for Surgical Resection: Although some cystic lesions of the pancreas, such as serous cystadenomas, can be managed conservatively, MCN are almost invariably resected when diagnosed. This strategy is supported by international guidelines (Fukuoka, AGA, European evidence-based guidelines) that recommend surgery, particularly in the presence of symptoms, mural nodules, or when the diagnosis of MCN is established. The risk of malignant transformation justifies this approach, even for relatively small lesions.
The Role of Spleen Preservation: Splenectomy, historically performed with distal pancreatectomy, carries well-established risks. Overwhelming post-splenectomy infection (OPSI), while rare (0.23% annual incidence), is associated with a very high mortality (38-69%) and can occur many years after splenectomy. The risk is particularly pronounced in younger patients, who must undergo lifelong preventive measures such as repeated vaccinations, prophylactic antibiotics during febrile episodes, and in some cases, prolonged antibiotic prophylaxis. By preserving the spleen, surgeons can mitigate these risks and maintain the immunological and hematological functions of the spleen.
Surgical Techniques for Spleen Preservation: Two main approaches are described for spleen-preserving distal pancreatectomy (SPDP). The Kimura technique involves meticulous dissection of the splenic artery and vein, preserving their continuity, providing excellent splenic perfusion but technically demanding. The Warshaw technique, on the other hand, involves resection of the splenic vessels while relying on short gastric and gastroepiploic vessels to maintain splenic perfusion. It is technically simpler and less hemorrhagic but carries a higher risk of splenic infarction, gastric varices, and secondary splenectomy. Comparative studies show Kimura’s approach reduces ischemic complications while Warshaw’s simplifies the procedure.
Minimally Invasive Approach: Laparoscopic distal pancreatectomy has facilitated adoption of spleen-preserving techniques, offering reduced pain, shorter stay, and faster recovery. When performed by experienced surgeons, laparoscopic SPDP achieves similar oncological outcomes compared with open surgery.
Oncological Safety: Complete resection with negative margins (R0) remains the cornerstone of MCN management. When the splenic vessels are preserved and radicality is respected, spleen-preserving pancreatectomy provides equivalent oncological outcomes to splenectomy. Long-term follow-up has demonstrated excellent prognosis for non-invasive MCN with negligible recurrence.
Implications for Clinical Practice: The decision between splenectomy and SPDP must be individualized, taking into account tumor location, vascular involvement, and surgical expertise. In the absence of splenic hilum invasion or major vessel encasement, SPDP should be favored for its morbidity reduction and immunological benefits.
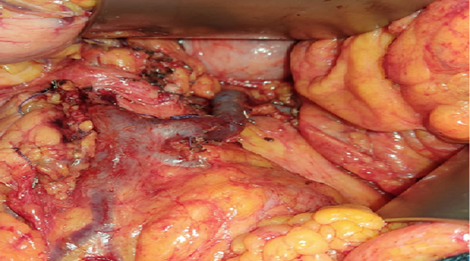
Figure 1: Distal Pancreatectomy with Spleen Preservation.

Figure 2: Surgical Specimen of Distal Pancreatectomy.
Conclusion
Spleen-preserving distal pancreatectomy is a valuable surgical approach for mucinous cystic neoplasms located in the pancreatic body and tail. It minimizes the risk of long-term infectious complications, avoids unnecessary splenectomy, and ensures oncological radicality in selected patients.
Declarations
Conflict of Interest
There are no potential competing interests.
Ethical Consideration
All the data collected and patient accepted to publish the case.
Acknowledgements
All the authors equally contributed for the case study.
References
- Tanaka, M., Fernández-del Castillo, C., Kamisawa, T., Jang, J. Y., Levy, P., et al. (2017). Revisions of International Consensus Fukuoka Guidelines for the Management of IPMN of the Pancreas. Pancreatology, 17(5):738-753.
Publisher | Google Scholor - Elta, G. H., Enestvedt, B. K., Sauer, B. G., Lennon, A. M. (2018). ACG Clinical Guideline: Diagnosis and Management of Pancreatic Cysts. Official journal of the American College of Gastroenterology (ACG), 113(4):464-479.
Publisher | Google Scholor - Kimura, W., Moriya, T., Ma, J., Kamio, Y., Watanabe, T., et al. (2007). Spleen-Preserving Distal Pancreatectomy with Conservation of the Splenic Artery and Vein. World Journal of Gastroenterology, 13(10):1493.
Publisher | Google Scholor - Warshaw, A. L. (1988). Conservation of the Spleen with Distal Pancreatectomy. Archives of Surgery, 123(5):550-553.
Publisher | Google Scholor - Shoup, M., Brennan, M. F., McWhite, K., Leung, D. H., Klimstra, D., et al. (2002). The Value of Splenic Preservation with Distal Pancreatectomy. Archives of surgery, 137(2):164-168.
Publisher | Google Scholor - Kang, C. M., Kim, D. H., Lee, W. J. (2010). Ten Years of Experience with Resection of Left-Sided Pancreatic Ductal Adenocarcinoma: Evolution and Initial Experience to A Laparoscopic Approach. Surgical Endoscopy, 24(7):1533-1541.
Publisher | Google Scholor - Venkat, R., Edil, B. H., Schulick, R. D., Lidor, A. O., Makary, M. A., et al. (2012). Laparoscopic Distal Pancreatectomy is Associated with Significantly Less Overall Morbidity Compared to The Open Technique: A Systematic Review and Meta-Analysis. Annals of Surgery, 255(6):1048-1059.
Publisher | Google Scholor - Sahakyan, M. A., Kazaryan, A. M., Rawashdeh, M., Fuks, D., Shmavonyan, M., et al. (2016). Laparoscopic Distal Pancreatectomy for Pancreatic Ductal Adenocarcinoma: Results of A Multicenter Cohort Study on 196 Patients. Surgical Endoscopy, 30(8):3409-3418.
Publisher | Google Scholor - Ferrone, C. R., Konstantinidis, I. T., Sahani, D. V., Wargo, J. A., Fernandez-del Castillo, C., et al. (2011). Twenty-Three Years of The Warshaw Operation for Distal Pancreatectomy with Preservation of The Spleen. Annals of Surgery, 253(6):1136-1139.
Publisher | Google Scholor - Sadot, E., Brennan, M. F., Lee, S. Y., Allen, P. J., Gönen, M., et al. (2014). Readmission After Pancreatic Resection: Causes and Causality Pattern. Annals of Surgical Oncology, 21(13):4342-4350.
Publisher | Google Scholor - Partelli, S., Cirocchi, R., Randolph, J., Parisi, A., Coratti, A., et al. (2016). A Systematic Review and Meta-Analysis of Spleen-Preserving Distal Pancreatectomy with Preservation or Ligation of The Splenic Artery and Vein. The Surgeon, 14(2):109-118.
Publisher | Google Scholor - Satoi, S., Yanagimoto, H., Yamamoto, T., Ohe, C., Miyasaka, C., et al. (2017). Clinical Outcomes of Pancreatic Ductal Adenocarcinoma Resection Following Neoadjuvant Chemoradiation Therapy vs. Chemotherapy. Surgery Today, 47(1):84-91.
Publisher | Google Scholor























