

Case Report
Skin as the First Frontier: A Rare Case of Cutaneous Metastasis in Breast Carcinoma
- Aiusee Nasreen Pooja *
Resident, Jawaharlal Nehru Medical College, Belgaum, Karnataka, India.
*Corresponding Author: Aiusee Nasreen Pooja, Resident, Jawaharlal Nehru Medical College, Belgaum, Karnataka, India.
Citation: Aiusee N. Pooja. (2024). Skin as the First Frontier: A Rare Case of Cutaneous Metastasis in Breast Carcinoma, International Journal of Clinical and Surgical Pathology, BioRes Scientia Publishers. 2(1):1-3. DOI: 10.59657/3067-0462.brs.25.013
Copyright: © 2025 Aiusee Nasreen Pooja, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: April 10, 2025 | Accepted: June 10, 2025 | Published: June 16, 2025
Abstract
Background: Cutaneous metastases can have variable clinical appearances and can mimic benign skin lesions. Cutaneous metastasis from breast cancer without direct involvement of skin by the underlying tumor is rare.
Case Presentation: A 47-year-old female presented with diffuse swelling of bilateral breast along with plaque on right breast and fluid filled vesicles on the chest. Histopathological examination of the skin lesions showed features of adenocarcinoma. Subsequently, core biopsy from the breast swellings revealed features of invasive breast carcinoma, not otherwise specified. Unfortunately, the patient did not survive after receiving one cycle of chemotherapy.
Conclusion: Cutaneous metastases of breast cancer, though infrequent, signify a bleak outlook for the patient and may be the first presenting feature, as was in this case. The importance of a comprehensive approach in dealing with the potential advancement of the disease cannot be overstated, underscoring the need for prompt diagnostic measures.
Keywords: breast cancer; histopathological examination; 47-year-old female
Introduction
Cutaneous metastasis manifests as migration of the malignant cells from their primary site to invade and colonize the skin [1]. Within the spectrum of cancer, metastasis is often viewed as the most destructive facets of malignancy. It may present as the first clue of an undetected internal malignancy or as the initial indication of dissemination, or even as the earliest sign of cancer recurrence [2]. In patients of breast carcinoma, the incidence of cutaneous metastasis is 23.9% [3]. General clinicians should be cognizant of this rare presentation as in our case of cutaneous metastasis of breast cancer which happened to be the first sign of the tumour disease.
Case Report
A 47-year-old female presented with blisters on chest and right breast. The lesion first started one and half years back which gradually increased in number. Patient came to our department for FNAC for suspected lump in the bilateral breasts. But no underlying lump was palpable. So, punch biopsy was planned from the vesicles and plaque and the sample was sent to the department of Pathology. Subsequent histopathological examination of the punch biopsy specimens from both the sites showed tumour cells arranged in solid nests and cribriform pattern (Figure 1A and 1B). Individual tumour cells are round to oval with high N:C ratio and prominent nucleoli. Few of the tumour islands show comedo necrosis. Few vascular spaces show tumour emboli along with RBCs (Figure 1C and 1D). So, on histopathology, diagnosis of adenocarcinoma was given with possibility of cutaneous metastasis. On the basis of our histopathological diagnosis, core biopsy from bilateral breasts were performed, following which the diagnosis of invasive ductal carcinoma, NOS was confirmed.
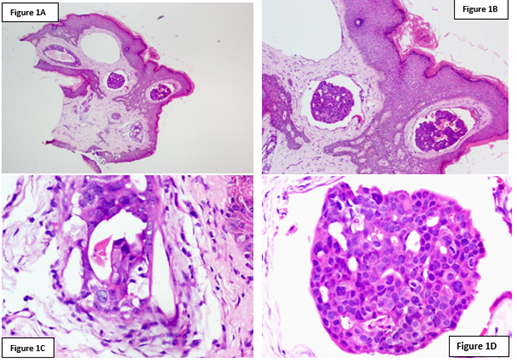
Figure 1: H&E pictomicrographs: A- Scanner image (4x) shows skin biopsy with nests of tumour cells in the dermis; B- Low power (10x) shows tumour cells arranged in nests and cribriform pattern; C & D- High power (40x) shows highly pleomorphic tumour cells with round to oval hyperchromatic nuclei, high N:C ratio and prominent nucleoli. Vascular spaces show tumour emboli along with RBCs.
On immunohistochemistry, the tumour cells from the breast cores expressed Her2 while being negative for ER and PR. The tumour cells from the vesicles and plaque expressed GATA3 and Her2 (Figure 2A and 2B). So based on the histomorphology and immunohistochemistry, a diagnosis of cutaneous metastatic carcinoma, also termed as carcinoma erysipeloides can be rendered.
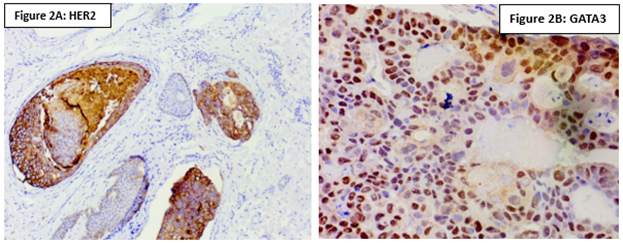
Figure 2: IHC analysis: A- HER2 positive; B- GATA3 positive.
Discussion
Skin changes as the first sign of breast cancer are uncommon and rarely observed in clinical settings. However, it's crucial to recognize that a non-specific skin lesion might mask an advanced cancer that can spread systemically before symptoms are apparent. This highlights the importance of considering malignancies as possible causes for persistent skin issues and incorporating them into the differential diagnosis [4]. Cutaneous metastases from primary internal malignancies are relatively rare, occurring in 0.7% to 10.4% of cases. The occurrence of cutaneous metastases in patients with breast carcinoma is 23.9% [5]. The lesions generally develop on the skin directly over or close to the site of the primary tumor, primarily due to the lymphatic dissemination of cancer cells [2]. Metastases to the skin can originate from various cancers, including carcinomas, melanomas, sarcomas, and hematologic malignancies. Adenocarcinomas make up roughly 60% of these cases. The primary sites most commonly associated with skin metastases are the breast, lung, and large intestine, while other, less frequent sources include the stomach, prostate, pancreas, ovary, endometrium, and thyroid [6]. Cutaneous metastases exhibit a broad spectrum of clinical manifestations in practice. While inflammatory breast cancer (carcinoma erysipeloides) and Paget’s disease of the nipple are more commonly known, nodules are the most typical presentation. In contrast, dermatitis-like metastases as the first indication of breast cancer are among the rarest forms, with only a single other case reported [7]. This uncommon presentation is highlighted by a retrospective analysis of 42 cases of skin metastases by Cidon, which revealed that just 7% were the first sign of tumor disease [8].
There are several morphological variants of cutaneous metastases, with the most common being solitary to multiple erythematous infiltrating papules and nodules. Rarer variants include carcinoma erysipeloides, carcinoma en cuirasse, carcinoma telangiectaticum, alopecia neoplastica, metastases to the inframammary crease, and a zosteriform pattern. There have also been reports of metastatic histiocytoid breast carcinoma presenting as painless eyelid swelling with nodular infiltration, metastatic masses resembling radiation dermatitis, and targetoid lesions. Most cutaneous metastases arise from the lymphatic spread of tumor cells. Histological variants include glandular patterns, the Indian file pattern of malignant cells between collagen fibers, lymphatic embolization by malignant cells, and fibrotic or epidermotropic patterns. The prognosis generally depends on the type and behavior of the primary tumor, with expected survival typically less than one year at the time of diagnosis [9]. Carcinoma erysipeloides, or inflammatory skin metastasis, is a relatively uncommon form of metastatic disease, representing less than 1% of all metastases and is typically linked to intraductal breast carcinoma [9]. Histopathological analysis of a biopsy can substantiate the diagnosis of cutaneous metastasis from breast carcinoma by showing malignant cells consistent with the primary tumor. Immunohistochemical staining, especially with Cathepsin D, which is predominantly expressed in breast carcinoma metastases, is important for diagnostic accuracy. Other markers such as pan cytokeratins, epithelial membrane antigen, and carcinoembryonic antigen are frequently positive, and immunoreactivity for androgen receptors in the metastatic tumor supports the diagnosis of a primary breast carcinoma [10]. A patient’s prognosis with cutaneous metastasis primarily depends on the type and aggressiveness of the primary tumor and its reaction to therapeutic interventions. Although, skin metastases from breast cancer often manifest at advanced disease stages and tend to be poorly responsive to treatment.
Conclusion
Cutaneous metastases from breast carcinoma occur in up to 23.9% of cases, with presentations ranging from the more common papulonodular forms to rare instances like dermatitis-like metastases. It is crucial for clinicians to recognize such rare presentations and conduct a comprehensive clinical, radiological, and histological evaluation (triple assessment) to achieve an accurate diagnosis and ensure timely and appropriate management.
References
- El Khoury, J., Khalifeh, I., Kibbi, A. G., Abbas, O. (2014). Cutaneous Metastasis: Clinicopathological Study of 72 Patients from A Tertiary Care Center in Lebanon. International Journal of Dermatology, 53(2):147-158.
Publisher | Google Scholor - Naser, A. M. B., Zaki, M. S., Brunner, M., Wollina, V., Zouboulis, C. C. (2007). Cutaneous Metastasis in Internal Malignancy. Egyptian Dermatol Online J, 3:1.
Publisher | Google Scholor - Schwartz, R. A. (1995). Cutaneous Metastatic Disease. Journal of the American Academy of Dermatology, 33(2):161-185.
Publisher | Google Scholor - Tahhan, N. K., Abou Azan, A., Al Ali, I. J., Aziz, J. A., Sara, S. (2023). Cutaneous Metastases as a Primary Manifestation of Invasive Ductal Carcinoma of The Breast: A Case Report. Annals of Medicine and Surgery, 85(6):3062-3065.
Publisher | Google Scholor - Lookingbill, D. P., Spangler, N., Helm, K. F. (1993). Cutaneous Metastases in Patients with Metastatic Carcinoma: A Retrospective Study of 4020 Patients. Journal of the American Academy of Dermatology, 29(2):228-236.
Publisher | Google Scholor - Araújo, E., Barbosa, M., Costa, R., Sousa, B., Costa, V. (2020). A First Sign Not to Be Missed: Cutaneous Metastasis from Breast Cancer. European Journal of Case Reports in Internal Medicine, 7(1):001356.
Publisher | Google Scholor - Ai‐ping, F., Yue, Q., Yan, W. (2007). A Case Report of Remote Cutaneous Metastasis from Male Breast Carcinoma. International Journal of Dermatology, 46(7):738-739.
Publisher | Google Scholor - Cidon, E. U. (2010). Cutaneous Metastases in 42 Patients with Cancer. Indian Journal of Dermatology, Venereology and Leprology, 76:409.
Publisher | Google Scholor - Prabhu, S., Pai, S. B., Handattu, S., Kudur, M. H., Vasanth, V. (2009). Cutaneous Metastases from Carcinoma Breast: The Common and The Rare. Indian Journal of Dermatology, Venereology and Leprology, 75:499.
Publisher | Google Scholor - Ahmed, M. (2011). Cutaneous Metastases from Breast Carcinoma. Case Reports, bcr0620114398.
Publisher | Google Scholor























