

Research Article
Human Papilloma Virus Related Knowledge and Attitude Among Women Participating in Cancer Screening in a Semi-rural Health District of the Republic of Cameroon
- Sylvester Adeh Nsoh 1
- Freddy Elad Essogmo 1,2
- Mosse B. A. Wilfried 1
- Che Joe Brown 1
- Isabella Fri Tayong 1,2
- Mary R. Nittala 3
- Paul Mobit 1,2,3
1Cameroon Oncology Center, P.O. Box 1882, Douala, Cameroon.
2Cameroon Cancer Foundation, Douala, Cameroon.
3Department of Radiation Oncology, University of Mississippi Medical Center, Jackson MS, United States of America.
*Corresponding Author: Paul Mobit, Department of Radiation Oncology, University of Mississippi Medical Center, Jackson MS, United States of America
Citation: Sylvester A. Nsoh, Freddy E. Essogmo, M.B.A. Wilfried, Che J. Brown, Mobit P, et al. (2025). Human Papilloma Virus Related Knowledge and Attitude Among Women Participating in Cancer Screening in a Semi-rural Health District of the Republic of Cameroon. Journal of Cancer Management and Research, BioRes Scientia Publishers. 3(1):1-7. DOI: 10.59657/2996-4563.brs.25.020
Copyright: © 2025 Paul Mobit, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: April 08, 2025 | Accepted: May 02, 2025 | Published: May 09, 2025
Abstract
Purpose and Objective(s): This was a descriptive cross-sectional study to determine the HPV-related knowledge and attitude and measure the level of acceptance of the HPV-vaccine amongst inhabitants of the health district of Dibombari located in Moungo Division, Littoral Region of the Republic of Cameroon.
Materials and Methods: This research was conducted with a high level of thoroughness. Participants were attendees of a free cancer screening campaign, a unique intervention planned and implemented by the Cameroon Oncology Center (COC) as part of the 2023 Breast Cancer Awareness Month activities. Screening was conducted in COC, places of worship, and community centers in and around the Dibombari Health District in the Republic of Cameroon. Each participant completed a self-administered questionnaire that sought to answer some HPV-related questions. In most cases, participants first listened to health talks before focusing on the questionnaires and screening.
Results and Conclusion: A total of 181 women participated in the study. Out of this number, 38.7% of the participants had post-high school diplomas, only about 28.9% had heard about HPV and the HPV vaccine, a large majority (63.8%) knew that cancer is preventable, 42.2% accepted to allow their children to receive the HPV vaccine while 42.8% of the study participants have once been diagnosed with genital warts. Given that at least 83.2% of the study participants had secondary school education or beyond, it was rather surprising that 71.1 % of the women had never heard about HPV or the HPV vaccine. This underscores the need for effective population-based sensitization campaigns.
Keywords: human papilloma; virus; women; cancer screening; Cameroon
Introduction
Cancer is a major public health problem in sub-Saharan Africa (SSA) and causes a significant percentage of premature deaths in adults between 30-69 years old [1]. New cancer cases were estimated to be over 800,000 in 2022 by the International Agency for Research on Cancer [2] and this number will grow to over 1.2 million in 2030. The total number of cancer cases in SSA is just an estimate because SSA lacks suitable cancer registries with trained staff. Most cancers are not diagnosed and even for the diagnosed, there is insufficient coordination of data sources. The rise in cancer incidence in SSA and other developing countries has been attributed to an increased life expectancy, lifestyle changes, and improved treatment of infectious diseases [3]. Contained in this cancer burden are cancers of the cervix, anus, penis, vulva, vagina, and oropharynx which are a group of cancers sharing a common causal link [4].
While anal, penial, vulvar, and vaginal cancers are rare [5,6,7], cervical cancer is a major public health problem globally with 560,000, new cases and about 275,000 deaths recorded each year, developing countries taking more than 55% of the mortality burden [8]. Cervical cancers is among the most common gynecological cancer in sub-Saharan Africa, with Cameroon, not spared [9]. Even though some cervical cancer screening programs have been implemented [10], current estimates indicate that every year, 2770 women are diagnosed with cervical cancer in Cameroon and 1787 die from the disease [11]. Cervical cancer is the second most frequent cancer among women between 13 and 44 years old in the general population of Cameroon, with a mortality-to-incidence rate greater than 65%, which raises this cancer to a public health concern [12]. Meanwhile, among the rare HPV-related cancers, 36068 new cases of penial cancer with 13,211 deaths were reported in 2020 [13].
World-wide, epidemiological, molecular, and clinical evidence has shown that cervical cancer is caused by the Human Papillomavirus (HPV), a sexually transmitted infection, especially serotypes 6, 11, 16, and 18 [14,15]. Growing evidence has established a causal link between HPV and other anogenital cancers (anus, vulva, vaginal and penis) and head and neck cancers [16,4]. HPV types 16 and 18 are responsible for about 70% of all cervical cancer cases world-wide (Bruni el, 2023) [16]. HPV has not been left out in the increased incidence of squamous cell carcinoma of the aerodigestive tract [4]. An estimated 85,000 cases of oropharyngeal cancer occurred worldwide in 2008, and at least 22,000 of these were HPV-positive [17].
First, discovered in skin cells in the 1950s, HPV is now understood to attack basal keratinocytes of the skin or mucosal membranes [18]. HPV is the most common STI in the world, particularly affecting sexually active adults and young women [19]. In Africa, about 3,8% of women in the general population are estimated to harbor cervical HPV-16/18 infection at any given time and 68.2 % of invasive cervical cancers are attributed to HPVs 16 or 18 [11]. Data on HPV in the general population is not yet available in Cameroon. However, ICO/IARC Information Center on HPV and Cancer posits that the crude incidence rates of HPV-related cancers among females in Cameroon are 20.9, 0,36, 0.39, 0.37, 0.21, 0.68, and 0.08, respectively, for cervical, anal, vulva, vaginal, oropharyngeal, oral cavity and laryngeal. Among males, these rates are 0,38, 0/08, 1.17, 1/04, and 0.23, respectively, for anal, penile, oropharyngeal, oral cavity, and laryngeal cancers.
Primary prevention of (HPV-related) cancers can be achieved through prevention and control of genital infection with oncotic HPV types [20]. The population’s HPV-related knowledge and attitude will undoubtedly be helpful to guide the planning and implementation of such interventions. This study’s primary objective was conducted by the Cameroon Oncology Center (COC), a privately owned but revenue-neutral modern oncology center located in the Dibombari health district, Republic of Cameroon. Dibomabri is one of about 360 smallest administrative units of the Republic of Cameroon and had a population of about 17,000 in 2005. Its population is estimated to be over 40,000 today. Dibombari is located to the north west of the city of Douala, which has an estimated population of over 4 million inhabitants and is the economic capital of Cameroon and the Central Africa sub region.
Materials
As in previous years, Cameroon Oncology Center (COC) celebrated Breast Cancer Awareness Month (October Rose) by performing free cancer screening not just for breast cancer but also for cervix and prostate. COC advertised the free cancer screening program through the district health office. Flyers and banners were prepared and posted throughout the district, advertising the month-long screening campaign. We also utilized the local community radio station to announce the free cancer screening campaign to the inhabitants of the health district. Announcements were also sent to local churches and other places of worship, fostering awareness and a sense of community involvement. The Regional Delegate of Health launched the cancer screening activities for the Littoral Region (the Littoral Region is an administrative unit equivalent to a state or province in other countries). The launching brought several national media houses, including TV, radio, and print media, further involving the community.
Most study participants were screened at the COC facility, but screening was also carried out in churches and several community centers around the health district, demonstrating the community’s active participation. The screening team was headed either by a gynecologist or radiation oncologist but occasionally by a general physician trained to perform the cancer screens. Participants were also screened for blood sugar levels and basic non-fasting cholesterol levels in addition to taking their blood pressure. The population was sensitized to come for screening during October free of charge. When screening was performed in our facility or community centers, participants in the screening activities must listen to a health talk about cancer delivered by the team leader for the screening event. The health talk on cancer included warning signs of breast cancer, rectal, prostate, and cervical cancers. Information on who to call or what to do if cancer is suspected. In addition, the “health talks” educated participants on the importance of maintaining a good social lifestyle and getting screened not just for cancer but for other non-communicable diseases such as high blood pressure and heart disease. Gender-specific education was offered on breast and cervical cancers for women and breast and prostate cancers for men, with a particular focus on self-examination. Each participant was first received by our trained nursing staff, who conducted a vital sign assessment and helped them complete the questionnaire shown in Figure 1. This questionnaire collected data participant’s general health, health knowledge, and relevant social and family history. The participant was then received by the person in charge of screening, who obtained informed consent after educating the participant on the procedure, including the benefits and possible discomforts.
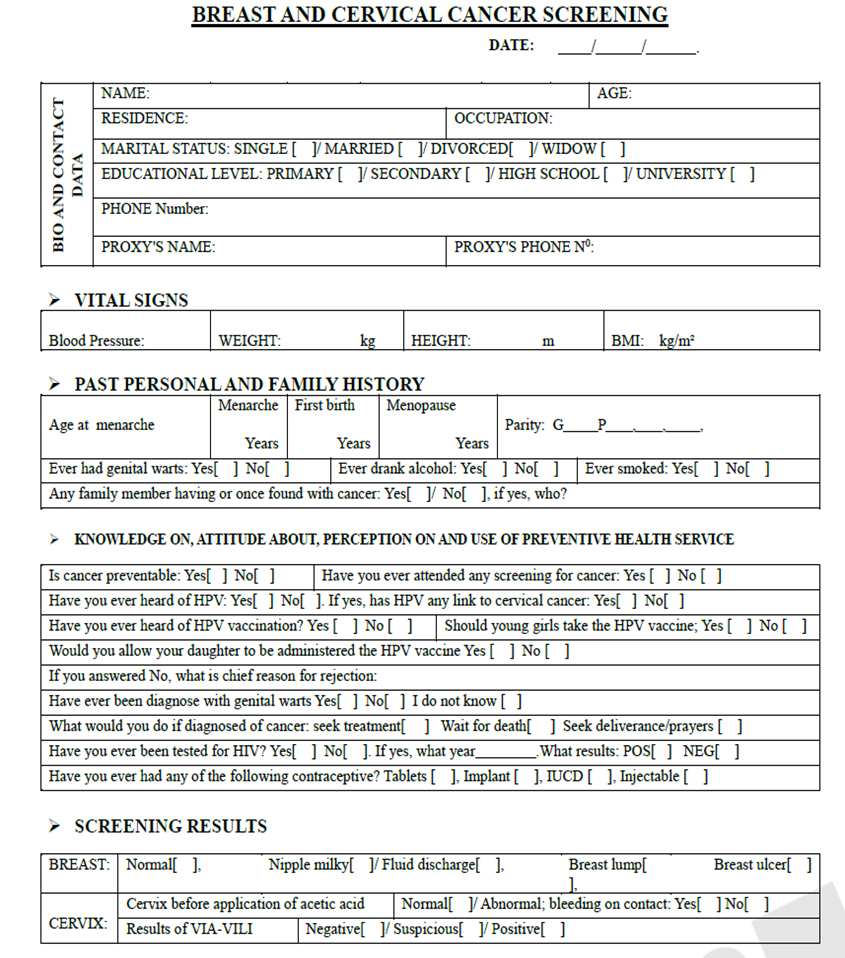
Figure 1: Questionnaire used by Cameroon Oncology Center for cancer screening campaign.
Results and Discussion
Sociodemographic Characteristics of Participants
A total of 181 women participated in the study screening. Section 1 of Table 1 shows the age distribution of the participants. Most of the participants (59 or 32.6%) were in the age group 40-49 years. Section 2 of the same table provides information on marital status, a significant variable in health status and outcomes. It was observed that, out of the 111 women with recorded marital status, a large majority (61 or 55%) were married. This finding is crucial for shaping health policies and interventions. Information on the highest level of education attained was recorded for 119 or 65.7% of the 181 participants. Section 3 of Table 1 details the distribution of the 119 women according to the highest level of education attained. Drawing from the table, a large majority (45 or 37.8%) of the women were university graduates. This high level of education may indicate a better understanding of the importance of cancer screening, leading to more proactive health behaviors for this educational cohort.
Table 1: Sociodemographic characteristics of Participant.
| Section | Variable | Category | Frequency | Percentage |
| Section 1 | Age range | 20-29 | 26 | 14.4 |
| 30-39 | 40 | 22.0 | ||
| 40-49 | 59 | 32.6 | ||
| 50-59 | 37 | 20.5 | ||
| 60-69 | 18 | 9.9 | ||
| 70-79 | 1 | 0.6 | ||
| TOTAL | 181 | 100 | ||
| Section 2 | Marital status | Single | 33 | 29.7 |
| Married | 61 | 55 | ||
| Divorced | 4 | 3.6 | ||
| Widow/widower | 13 | 11,7 | ||
| TOTAL | 111 | 100 | ||
| Section 3 | Highest educational level Attained | Not been to school | 0 | 0 |
| Primary | 20 | 16.8 | ||
| Secondary | 29 | 24.4 | ||
| High School | 25 | 21 | ||
| University | 45 | 37.8 | ||
| TOTAL | 119 | 100 |
Participants’ knowledge and attitude on HPV-related parameters and cancer preventability
Data to assess if participants had ever heard of the Human Papillomavirus (HPV) was recorded from 128(68.1%) of the 181 participants. Section 1 of Table 2 reveals that 91 or 71.1% of respondents had never heard of HPV. This high proportion of ‘Never heard of HPV’ responses had policy implications. Public health interventions should seek to address this knowledge gap. This means that only 37 study participants out of the 128 surveyed (20.4%) have some basic information about HPV. Data on awareness of a vaccine against HPV was obtained from 128 (70.1%) of the 181 participants. Section 3 of Table 2 distributes the participants according to the obtained responses. Almost three out of four participants who had a recorded response were not aware of the existence of a vaccine against HPV. This low awareness underscores the need for more effective campaigns to improve HPV vaccination awareness, fostering a sense of determination and commitment in the field of public health. Data assessing the participants’ knowledge of the preventability of cancer was recorded from 127 (70.2%) of the 181 participants. Section 4 of Table 2 distributes the participants according to their responses.
A large majority of the participants (63.8%) affirmed that cancer is preventable. This significant belief can serve as a powerful leverage for promoting cancer prevention services and instilling hope and motivation in the field of public health. A question was posed to ascertain any personal history of genital warts. Responses were obtained from 131 or 72.4 % of the 181 participants; section 4 of Table 2 shows that 42.8% of the respondents reported that they had once been diagnosed with genital warts. This underscores the need for effective strategies to increase clinical diagnostic skills and encourage laboratory testing, particularly for HPV strains with oncogenic propensity. As to immunological protection against HPV infection, a question was posed to ascertain the stance of the women towards offering their consent for the vaccination of girls aged 11-12 years old. Section 5 of Table 2 reveals that 128 or 68.1% of women responded to this question.
The majority (57.6%) of the respondents would not accept girls being vaccinated against HPV. This low acceptance rate is likely due to a lack of awareness about the vaccine’s benefits, concerns about safety, or cultural and religious beliefs. Understanding the specific reasons is crucial for designing effective vaccination promotional strategies.
Table 2: Distribution of participants according HPV-related variables.
| Section | Question | Answer | Frequency | Percentage |
| Section 1 | Have you ever heard of HPV? | Yes | 17 | 28.9 |
| No | 91 | 71.1 | ||
| TOTAL | 128 | 100 | ||
| Section 2 | Have you ever heard of HPV vaccine | Yes | 33 | 25.8 |
| No | 92 | 71.9 | ||
| Don’t know | 3 | 2.3 | ||
| TOTAL | 128 | 100 | ||
| Section 3 | Is cancer preventable? | Yes | 81 | 63.8 |
| No | 37 | 29.1 | ||
| Don’t know | 9 | 0.07 | ||
| TOTAL | 127 | 100 | ||
| Section 4 | Have you ever been diagnosed with genital warts? | Yes | 56 | 42.8 |
| No | 55 | 41.9 | ||
| Don/t know | 20 | 15.3 | ||
| TOTAL | 131 | 100 | ||
| Section 5 | Should girls 11-12 years of age take HPV vaccines? | Yes | 54 | 42.2 |
| No | 74 | 57.2 | ||
| TOTAL | 128 | 100 |
Discussion
The sample size of just 181 participants for the study was small. Given that the participants did not have to pay as the screening was free to participants, it was surprising that few individuals took advantage of the free cancer screening that was offered in multiple locations in and around the health district for an entire month. We expected a better turnout since screening was offered in churches and other places of worship, trusted by the population. The screening was opened for the entire month of October 2023, and the population was well-sensitized since we used the community radio, banderols at strategic junctions within the health district, church announcements and the office of the District Medical Officer (DMO), which uses additional distribution channels to pass on the message of free cancer screening. So, the population was well-sensitized to the free cancer screening campaign. In other regions of the country, for instance, in the West or North West region, we usually screened more than 200 participants in two consecutive days of screening. However, it should be noted that in the present study, most of the study participants have had at least one previous cancer screening, which may help explain the low participation rate in this health district. On the other hand, Teddyl et al. [21], 2015 in a similar study, collected data from 255 respondents in Abuja, Nigeria.
The data also indicates that 83.2% of the participants had at least secondary-level education., Most of the women were university graduates. We expected more participants from the lower educational level, but this was not the case in this health district as most screening participants were graduates. This finding is in sharp contrast to other regions where we have screened. In these regions, most participants have yet to have formal education, especially in the northern regions of Cameroon. In fact, 83.2% of the women had at least a secondary-level education. This approximates 90% as found by Teddyl et al. [21] in 2015 in Abuja, Nigeria.
Regarding the key variable of knowledge on HPV, most of the study participants lack knowledge.
Of the 181 participants, only 128(70.7%) answered the question. It is possible that the respondents who failed to answer the question did so because they had truly never heard of HPV. Of the 128 women who responded to the question, 91(71.1%) reported that they had never heard of HPV, which is an alarming finding. Public health interventions need to develop appropriate message delivery strategies. However, this study found that 17(9.3%) of all respondents had heard of HPV. Teddyl et al. [21] found 9% in 2015 in Abuja, Nigeria. Out of the 128 women who provided information on the existence or not of the HPV vaccine, only 33(25.8%) affirmed the existence of the vaccine yielding Teddyl et al. [21], 2015 found a far lower percentage (7.8) in Abuja, Nigeria. Interestingly, out of the 131 women who responded to a question seeking to know if girls aged 11-12 years of age should receive the HPV vaccine, 56(42.8%) answered affirmatively, signaling a gap between knowledge and attitude on the HPV vaccine. Teddyl et al. [21], 2015 found 62.8% in their study. Even though the data was not stratified to ascertain the relationship between knowing the vaccine and positively consenting to HPV vaccination, bridging the gap may significantly raise acceptance of the vaccine, whose beneficial role in preventing cervical cancer has been well documented. Thinking in this direction should also leverage the additional findings in this study that 81 (63.8%) of 127 women believed that cancer is preventable, and 54(42.2%) of 128 women had once been diagnosed with genital warts. These findings should inform policy formulation and strategy development processes.
Conclusion
Awareness of the Human Papillomavirus (HPV) and the existence of a protective vaccine is low among cancer screening participants in the Dibombari Health District. When compared to the proportion of the study participants with knowledge of the existence of HPV and a vaccine against the virus, a relatively higher proportion of participants knew that cancer is preventable and were willing to allow their children to be vaccinated against HPV. These findings can significantly inform and boost policies and strategies if considered. The higher awareness of the preventability of cancer is a window of opportunity for interventions to increase the acceptance of the HPV vaccine. Effective sensitization campaigns are also needed to raise awareness of HPV and the existence of a protective vaccine. This approach which will undoubtedly have a significant positive impact on HPV vaccine acceptance. To have building blocks for developing such effective sensitization campaigns, other studies should be conducted to probe into the reason for the low awareness of HPV and the vaccine. By extension, the studies should address the reasons why some parents are unwilling to allow their children to receive the HPV vaccine. The output of these studies would serve in the reinforcement of vaccination efforts against HPV in the Dibombari Health District with a long-term decrease in the burden of HPV-related cancers.
Declarations
Conflicts of Interest
There are no conflicts of interest.
Ethical Approval
Not applicable.
Acknowledgments
The authors would like to acknowledge with thanks the staff of Cameroon Oncology Center for their contribution.
References
- Bray F, Parkin DM. (2022). African Cancer Registry Network. Cancer in sub-Saharan Africa in 2020: a review of current estimates of the national burden, data gaps, and future needs. Lancet Oncol, 23(6):719-728.
Publisher | Google Scholor - Bray F, Laversanne M, Weiderpass E, Soerjomataram I. (2021). The Ever-increasing Importance of Cancer as a Leading Cause of Death World-wide. Cancer, 127(16):3029-3030.
Publisher | Google Scholor - Bray F, Laversanne M, Sung H, Ferlay J, Siegel RL, Soerjomataram I, Jemal A. (2024). Global Cancer Statistics 2022. GLOBOCAN Estimates of Incidence and Mortality World-wide for 36 in 185 Cointries. CA Cancer J Clin, 74(3):229-263.
Publisher | Google Scholor - Kristen B. Plylynia, Kristina R Dahlstrom and Erich M Sturgis. (2014). Epidemiology of HPV-associated Oropharyngeal cancers. Oral Oncol, 50(5)380-386.
Publisher | Google Scholor - Cathy Eng, Kristen K Ciombor, May Cho, Jeniffer A Dorth, Lakshmi N Raidey, David P Horowitz, Mar J Gollab, Alexandre A Jacome, Natalie A Locknev, Robert L Muldoon, Mary Kav Washington, Brittany A O’Brian, Amula Benny, Cody M Lebeck Lee, Al B Benson, Karvin A, Goodman Van Karlyle Morris. (2022). Anal Cancer: Emerging Standars in a rare disease. J clin Oncol, 40(24).
Publisher | Google Scholor - Leiwen Fu, Tian Tian, Kai Yao, Xiang-Feng Chen, Guanfan Luo, Yingxiao Gao, Yi-Fan Lin, Bingyi Wang, Yinhsui, San Weiran Zhen, Chritopher K Pairley, Andrew Grulich, Huachun Zou. (2022). Global patterns and trends in Penile cancer Incidence: Population-based Study. JMIR Public Health and Surveillance, 8(7).
Publisher | Google Scholor - Mario Preti, Denis Querlau. (2022). Vulav Cancer: facing a Rare Disease. Cancers, 14(6):1581.
Publisher | Google Scholor - Ferlay J. Shin Hr, Bray F, Forman-D, mathers C, Parkin DM. (2010). Estimates of World Burden of Cancers, GLOBOCAN 2008. Int J. Cancer, 217:2893-2917.
Publisher | Google Scholor - Premilia Leiphrakpam, Chandrakanth Ave. (2024). Cancer on The Global Stage. Incidence and Cancer-related Mortality in Cameroon. WHO Regional Africa.
Publisher | Google Scholor - Sylvester Adeh Nsoh, Paul Mobit, Nicholas Ade, Mc Che Joe Brown, Ambe Yancho, Isabella Fri Tayong. (2022). Design and Implementation of a Cancer Screening Program for a Health District in Sub-Saharan Africa: A Pilot Study. International Journal of Clinical Oncology and Cancer Research, 10(4):83-88.
Publisher | Google Scholor - ICO/IARC information Center on HPV and Cancers. Cameroon Human Papillomavirus and Related Cancers; Fact Sheets.
Publisher | Google Scholor - IARC, World Health Organization International Agency for Research on Cancer, 2021. GLOBOCAN 2020: Estimated cancer incidence, mortality and prevalence worldwide in 2020.
Publisher | Google Scholor - Louie KS, de Sanjose S, Mayaud P. (2009). Epidemiology and Prevention of Huma Papillomavirus and Cancer in Subsaharan Africa: A Comprehensive review. Trop med Int Health, 14:1287-1302.
Publisher | Google Scholor - Prat J. (2012). Pathology of Cancers of the Female Gebital Tract. Int J. Gynecol. Obstet, 119:S137-150.
Publisher | Google Scholor - Pantawala IY, Bauer HM, Miymoto J, Park IU, Hucko MJ, Smith-MCCune KK. (2013). A Systematic Review of Randomised Trials Assessing Human Papillomavirus Testing in Cervical Cancer Screening. Am J Obst Gynecol, 208:343-355.
Publisher | Google Scholor - Bruni L, Albero G, Sewano B, Mena M, Colado JJ, Gomez D, Monoz J, Boseh FX, De Sanjose S. (2023). ICO/IARC Information Center on HPV and Cancer (HPV Information Center). Human Papillomavirus and Related Diseases, Summary Report.
Publisher | Google Scholor - De Martel C, George D, Bray F, Farley J, Clifford GM. (2020). Global Burden of Cancer attributable to Infections in 2018: a World-wide incidence Analysi. Lancet Glob Health, 8(2):e180-e190
Publisher | Google Scholor - Hausen H. (1978). Condylomata accuminata and Human Genital cancers. Cancer Research, 36:794.
Publisher | Google Scholor - Akom E Venne. (2003). Sinstitut Nationale de Sante Publique du Quebec. L’infection au Virus du Papillome Humain (VPH); Institute national de Sante de Quebec.
Publisher | Google Scholor - Franco EL, Harper DM. (2005). Vaccination Against Human Papillomavirus Infection: A New Paradigm in Cervical Cancer Control. Vaccine, 23:2388-2394.
Publisher | Google Scholor - Teddy E Agida, Godwin O Akaba, Aliyu Y Esah, Bissalla Ekele. (2015). Knowledge and Perceptions of the Human Papillomavirus Vaccine Among Antenal Women in Nigeria Tertiary Hospital. Nigerian Med J, 56(1):23-27.
Publisher | Google Scholor























