

Clinical Image
Bizarre Case of Peritoneal CSF-Pseudocyst Provoking Hydronephrosis in A Patient with Ventricle-Peritoneal Shunt
Merit Health Wesley Health Center, Hattiesburg, MS, United States America.
*Corresponding Author: Sri Harsha Kanuri,Merit Health Wesley Health Center, Hattiesburg, MS, United States America.
Citation: Sri H. Kanuri, K Messenger. (2026). Bizarre Case of Peritoneal CSF-Pseudocyst Provoking Hydronephrosis in A Patient with Ventricle-Peritoneal Shunt. Journal of Neuroscience and Neurological Research. BioRes Scientia Publishers.5(2):1-3. DOI: 10.59657/2837-4843.brs.26.039
Copyright: © 2026 Sri Harsha Kanuri, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: December 08, 2025 | Accepted: February 18, 2026 | Published: February 27, 2026
Abstract
We report a case of a 51-year-old male presented to the neurology clinic with intermittent dizziness, blurred vision, chronic left sided weakness and numbness. He was previously diagnosed with Arnold Chiari type I malformation for which ventricle-peritoneal shunt was performed in 1994. Following this, ensuing imaging or evaluation of the shunt was never attempted. During routine follow up, he complained of abdominal pain and subsequent work up revealed microscopic hematuria. A CT scan of abdomen and pelvis unearthed an abdominal cerebrospinal fluid pseudocyst which is compressing the ureter and causing hydronephrosis. Subsequently, he was referred for surgical resection of abdominal pseudocyst, thus resolving his abdominal pain and hydronephrosis.
Keywords: arnold chiari malformation; ventricle-peritoneal shunt; neuropathy; ureteral obstruction; csf pseudocyst; microscopic hematuria and hydronephrosis
Clinical Image
Case presentation: We report a case of a 51-year-old male presented to the neurology clinic with intermittent dizziness, blurred vision, chronic left sided weakness and numbness. He was previously diagnosed with Arnold Chiari type I malformation for which ventricle-peritoneal shunt (VPS) was performed in 1994 (Figure 1). Following this, ensuing imaging or evaluation of the shunt was never attempted. During routine follow up, he complained of abdominal pain and subsequent work up revealed microscopic hematuria. A CT scan of abdomen and pelvis unearthed an abdominal cerebrospinal fluid (CSF) pseudocyst which is compressing the ureter and causing hydronephrosis (Figure 2). Subsequently, he was referred for surgical resection of abdominal pseudocyst, thus resolving his abdominal pain and hydronephrosis.
Discussion
There is an excess buildup of CSF in clinical disorders such as hydrocephalus, tumors, arachnoid cyst or myelomeningocele due to thwarting of CSF circulation in the brain [1]. Accordingly, increased intracranial pressure due to crippled CSF drainage can lead to symptoms ranging from chronic headaches, learning difficulties, visual disturbances, urinary retention, dementia, gait disturbances and mental retardation [1,2]. In such clinical scenarios, a VPS is a best therapeutic option to drain and divert the excess CSF from the cerebral ventricles to the abdominal cavity, atrial cavity or pleural cavity [1]. In patient with VPS, the risk of developing abdominal pseudocyst is heightened due to stymied CSF absorption in the peritoneal cavity secondary to infections, adhesions, subclinical peritonitis, obstruction, and multiple shunt revision [3]. Furthermore, foreign body reaction stimulating localized adhesions, inflammation and particle like proteins in the CSF are also speculated to be the possible mechanisms for CSF pseudocyst inception [4]. Moreover, shunt failure might happen due to proximal malfunction, distal failure, catheter occlusion and infection, thus inciting impaired CSF drainage and fluid accumulation in the gut [5].
Peritoneal CSF pseudocysts are broadly classified into three types according to their pathophysiological states, actively infected, sterile with active systemic inflammation, and sterile with no signs of systemic inflammation [6]. The incidence of abdominal pseudocyst is approximately 0.33-6.8% in patients with VPS shunt [7]. When such a clinical scenario transpires, the patient can present with abdominal pain, abdominal mass, nausea, vomiting, and headache. Very rarely, the CSF pseudocyst enlarges so that it can obstruct the ureter causing hydronephrosis and renal failure as happened in our patient [8]. Ultrasonography and CT (Computer Tomography) scan abdomen is usually diagnostic for diagnosis of peritoneal CSF pseudocyst [9]. Surgical therapy is the mainstay of management of peritoneal CSF pseudocyst. This entails redirection of shunt into different abdominal quadrant, atrial cavity or pleural cavity or external surface [10-12]. All the patients should be treated with empirical antibiotics irrespective of pseudocyst culture results, as subclinical infection can be commonly responsible for instigating recurrent CSF pseudocysts [6].
In our patient, CSF pseudocyst was surgically excised and shunt was repositioned to different abdominal quadrant. This resulted in significant relief of his signs and symptoms. Most cases of peritoneal pseudocyst occur within 6 months of previous abdominal surgery secondary to low grade infection, peritonitis or immune mediated reaction [11,13]. The presence of inflammatory markers requires external distal tubing with peritoneal reimplantation while absence of inflammatory markers necessitates reimplantation within the peritoneum [6]. 1-year survival rate of laparoscopic shunt diversion is poorer in infected pseudocysts (47%) as compared to non-infectious cases (100%) [6]. 1-year-survival rate in shunts managed with distal shunt externalization and distal shunt externalization followed by peritoneal reimplantation is 82% and 90% respectively [6,14].
Case highlights
In patients with VPS, a high degree of suspicion is necessary for peritoneal abdominal pseudocyst in those presenting with abdominal pain and abdominal swelling. Common causes of peritoneal CSF pseudocyst include infection, adhesions, previous abdominal surgery, foreign body reaction and immune mediated mechanism. Prompt confirmation of diagnosis with abdominal CT is required before moving forward with shunt explanation or revision. Treatment of infection is always required as subclinical infection can precipitate higher recurrence rates with associated increase in morbidity and mortality. Patients with VPS shunt should undergo regular follow up as shunt revision might be required as early as 5-10 years.
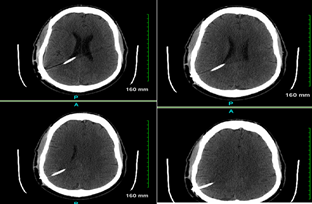
Figure 1: CT Head with and without contrast
A right posterior parietal approach shunt extending though the lateral ventricle with its tip at the posterior midline in the upper third ventricle. Ventricular system appears to be decompressed. The intracranial and extracranial shunt tube appears to be normal.
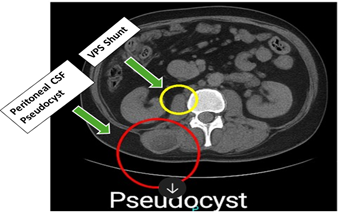
Figure 2: CT abdomen and pelvis
Imaging of the pelvis shows loculated fluid collection in the right lower quadrant. There are some calcifications in soft tissues in the right lower quadrant.
Declarations
Ethical Approval and Consent to participate
Not Applicable
Consent for publication
Consent taken
Availability of data and materials
Not Applicable
Competing interests
Not Applicable
Funding
Not Applicable
Acknowledgements
Not applicable.
Authors' contributions
Conceptualization, S.H.K & KM; Methodology, S.H.K & KM; Software, N.G.; Validation, N.A; Formal Analysis, N.A.; Investigation, S.H.K & VP.; Resources, N.A.; Data Curation, N.A.; Writing– Original Draft Preparation, S.H.K & KM.; Writing– Review & Editing, S.H.K.& KM.; Visualization, S.H.K.; Supervision, K.M..; Project Administration, K.M.
References
- Fowler JB, D. J. O., Mesfin FB. (2025 ).
Publisher | Google Scholor - Erps, A., et al. (2018).
Publisher | Google Scholor - Fatani, G. M., et al. (2020).
Publisher | Google Scholor - Yim, S. B., et al. (2018).
Publisher | Google Scholor - Stone, J. J., et al. (2013).
Publisher | Google Scholor - Whittemore, B. A., et al. (2024).
Publisher | Google Scholor - Yim, S. B., et al. (2018).
Publisher | Google Scholor - Mobley, L. W., 3rd, et al. (2005).
Publisher | Google Scholor - Leung, G. K. K. (2010).
Publisher | Google Scholor - Egelhoff, J., et al. (1985).
Publisher | Google Scholor - Erşahin, Y., et al. (1996).
Publisher | Google Scholor - Yuh, S. J. and M. Vassilyadi (2012).
Publisher | Google Scholor - Gaskill, S. J. and A. E. Marlin (1989).
Publisher | Google Scholor - Raghavendra, B. N., et al. (1981).
Publisher | Google Scholor - Erwood, A., et al. (2020).
Publisher | Google Scholor























