

Case Report
Angiographically Detected Coronary Artery Disease Concomitant with Myocardial Bridging-Treatment Strategy: A Case Report
1Associate Consultant, Department of Cardiac Surgery, Square Hospitals Limited, Dhaka, Bangladesh.
2Junior Consultant, Department of Cardiac Surgery, Square Hospitals Limited, Dhaka, Bangladesh.
3Associate Consultant, Department of Cardiac Anaesthesia, Square Hospitals Limited, Dhaka, Bangladesh.
4Specialist, Department of Cardiac Anaesthesia, Square Hospitals Limited, Dhaka, Bangladesh.
5Assistant Professor, Department of Cardiology, Bangladesh Medical University, Dhaka, Bangladesh.
6Consultant, Department of Cardiac Surgery, Lab Aid Cardiac Hospital, Dhaka, Bangladesh.
*Corresponding Author: Sultan Sarwar Parvez, Associate Consultant, Department of Cardiac Surgery, Square Hospitals Limited, Dhaka, Bangladesh.
Citation: Parvez SS, Bari N, Haider A, Saha A, Salam A, et al. (2025). Angiographically Detected Coronary Artery Disease Concomitant with Myocardial Bridging-Treatment Strategy: A Case Report, Journal of Clinical Cardiology and Cardiology Research, BioRes Scientia Publishers. 4(2):1-8. DOI: 10.59657/2837-4673.brs.25.051
Copyright: © 2025 Sultan Sarwar Parvez, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: June 23, 2025 | Accepted: July 15, 2025 | Published: July 21, 2025
Abstract
Myocardial bridging is a congenital anatomical variant in which a segment of epicardial coronary artery runs within the myocardium instead of normal course on the epicardial surface that becomes compressed during systole. Myocardial bridges can be classified in different ways. The length and thickness to which it covers the artery determines the degree of myocardial bridging. It can be symptomatic or asymptomatic. The mid segment of the left anterior descending (LAD) coronary artery is where myocardial bridging most frequently occurs. Development of atherosclerosis can be associated with myocardial bridging in same coronary artery proximal to the bridging segment with atherosclerosis of another coronary artery without myocardial bridging or atherosclerosis of one coronary artery with myocardial bridging of another coronary artery. After evaluation for diagnosing of myocardial bridge, it can be treated either with medical management, coronary stenting, or surgical intervention.
Keywords: myocardial bridging; surgical unroofing; coronary artery disease; coronary angiography
Introduction
Myocardial bridging is a congenital anatomical variation of a cardiac condition in which an overlaying band of muscle (myocardium) compresses a portion of the tunnelled coronary artery during systole and disappears completely during diastole [1]. Since the sixteenth century, myocardial bridging has been well recognized anatomically [2]. Usually, myocardial bridging is asymptomatic but when the segment of tunnelled coronary artery is compressed by overlying bridge muscle, it may cause ischemic sign and symptoms, such as angina, coronary spasm, arrhythmia, myocardial infraction, syncopal attack, Left ventricular dysfunction, even sudden cardiac arrest and death [3,4]. In 1737, Reyman was first discovered myocardial bridging (MB) during an autopsy [5] and angiographically first detected by Porstmann and Iwig in 1960 [6]. Myocardial bridge can occur both in male and female but in female is more predominant. Different diagnostic tools yield different prevalence rates for myocardial bridge (MB). Coronary angiographically myocardial bridge ranging from 0.5 to 12%, on autopsy and coronary computed tomography angiographically this rate reported 86% and 25% respectively [7]. The middle segment of the left anterior descending (LAD) coronary artery is where myocardial bridging most frequently occurs (77.2%). Then it occurs in left circumflex artery (40%) and the right coronary artery (36%) [8].
Ferreria et al. [9] divided the myocardial bridging of the LAD artery pathologically into two types: (1) Superficial bridges (more common, approximately 75%) situated intraventricular groove but crossed by a bundle of muscle perpendicularly or at an acute angle (2) Deep bridges in which the LAD artery deviates toward the right ventricle. Superficial bridging does not hamper coronary blood flow during systole, whereas deep bridges compress the coronary artery during systole reduces coronary blood flow and induces myocardial ischemia. This classification depends on the length and thickness of the overlying muscle band. Usually, myocardial bridge length is reported at 10-30mm and its depth is typically stated as 1-10 mm [10]. Development of atherosclerosis can be associated with myocardial bridging in same coronary artery proximal to the bridging segment, or with atherosclerosis of another coronary artery without myocardial bridging. The development of coronary atherosclerosis and coronary heart disease should be considered as independent risk factors for myocardial bridging [11]. While myocardial bridges in the coronary arteries are generally thought to be benign conditions, some studies have shown that they can cause angina pectoris, acute coronary syndrome, ventricular arrhythmia, left ventricular dysfunction, and even sudden cardiac arrest and death [12]. Because of changes in flow patterns, the area of the artery closest to the bridge may be more susceptible to atherosclerosis. The bridge segment's endothelial dysfunction predisposes it to coronary spasm [13,14].
Myocardial bridging can be diagnosed by different modalities like coronary angiography, multidetector computed tomography (MDCT) test, multislice CTA, intravascular ultrasound (IVUS), stress echocardiography but coronary angiography has more diagnostic value. Treatment options of myocardial bridging with coronary artery disease included medical management, coronary stenting, and surgery but which is appropriate? Here we report a case of angiographically detected coronary artery disease concomitant with myocardial bridging requiring coronary artery bypass surgery with surgical myotomy or unroofing of myocardial bridge.
Case Report
A 61-Year-old male had complaints of chest pain associated with shortness of breath and history of syncopal attack about 6 months back. Then he was initially admitted to a local hospital where ECG & Echo were done and diagnosed as OMI(Inferior). Since then, he was on regular medications and was relatively well and discharged with advice for coronary angiography. After that, he was admitted to a cardiac center for doing coronary angiography and diagnosed as single vessel coronary artery disease with long segment myocardial bridge in mid segment of LAD. PCI to RCA was attempted in same sitting but it was failed and then he was recommended for coronary artery bypass surgery but patient was discharged on request at that time. After that he had experienced frequent breathlessness and palpitation for 2 days at home and with these problems, he was admitted to our cardiac surgery department through outpatient department for coronary artery bypass surgery.
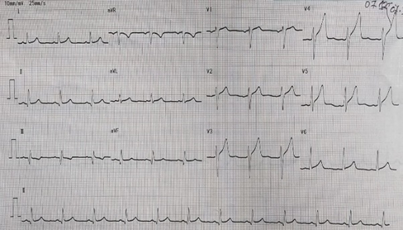
He had history of diabetes mellitus, systemic arterial hypertension, bronchial asthma, and skin allergy. He was non-smoker, non-alcoholic and had no history of similar diseases and genetic disorders but had history of coronary artery disease in his family. On physical examination, pulse rate was 88 beats/min, blood pressure was 120/80 mmhg, respiratory rate was 22/min, SpO2 was 97% on room air. Electrocardiogram (ECG) showed Old MI(Inferior).
Cardiac enzymes were normal. All biochemical investigations were within normal limit. Chest x-ray P/A view shows normal findings.
Figure 2: X-ray Chest P/A view showing normal findings.
Echocardiogram showed basal inferior-infer septum, mid basal posterolateral wall moderately with mild mid anteroseptal - anterior wall hypokinesia, mild to moderate LV systolic dysfunction (EF:40-45%), mitral regurgitation, normal RV function.
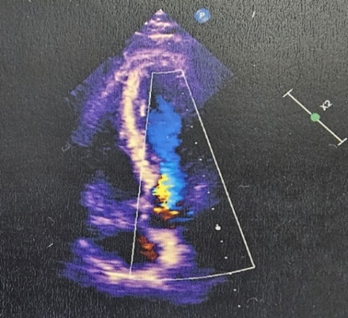
Figure 3: Echocardiography showing mild regurgitation with hypokinesia with mild to moderate LV dysfunction.
Coronary angiography showed single vessel coronary artery disease with long segment myocardial bridge in mid LAD, RCA-Totally occluded from its ostial part with retrograde filling by left system.
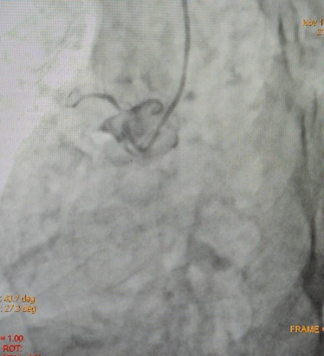
Figure 4: RCA-Totally occluded from its ostial part.

Figure 5: Failed PCI to RCA.

Figure 6: Long segment myocardial bridge in mid LAD (Milking Effect), during systole.

Figure 7: Long segment myocardial bridge in mid LAD during diastole.
The patient was denied to do Intravascular Ultrasound (IVUS) and Fractional Flow Reserve (FFR) assessment. So, after evaluation of the patient, he was sent to the operating room for coronary artery bypass surgery with unroofing of myocardial bridge in mid LAD. Surgery was performed with endotracheal intubation under G/A and with median sternotomy. After median sternotomy, pericardiotomy was done. Aorta showed healthy, PA (Pulmonary Artery) showed mildly tense, LV-Normal. Cardiopulmonary Bypass was established with aortic and dual stage venous cannulation. At first on pump beating heart, RSVG (Reverse saphenous venous graft) to PDA, distal grafting was done with prolene 7/0.
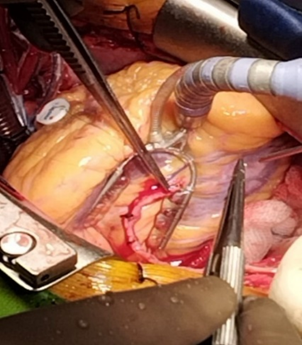
Figure 8: RSVG to PDA graft.
Then aorta was cross clamped and heart was arrested with antegrade cold-blood cardioplegia. After that to inspect epicardial surface of heart for intramyocardial LAD, was easily detected. Epicardial incision was given over the normal site of LAD coronary artery with 15 size surgical blade. Then dissection was extended proximally into the bridging portion of LAD coronary artery with the dissection of epicardial fat and underlying muscle or myocardial bridge with the help of Potts scissors and Electrocautery. The length of the myocardial bridge was about 4.5 cm. Careful dissection was done to avoid damage to the LAD coronary artery and its branches such as diagonal artery and to avoid injury to right ventricle. During dissection of epicardial fat and outer part of myocardial bridge electrocautery or Liga clip were used for hemostatic purpose.
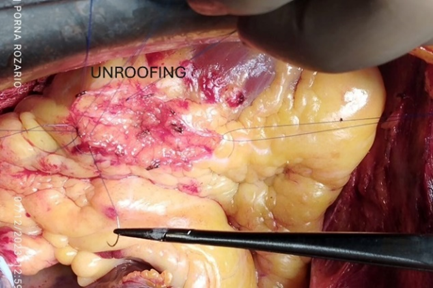
Figure 9: Surgical Unroofing of Myocardial Bridge with exposed LAD artery.
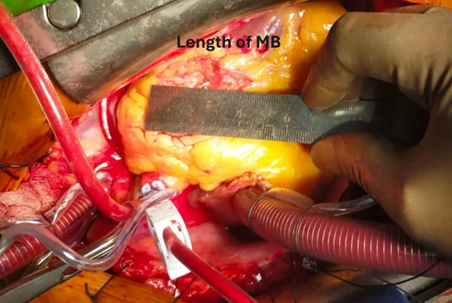
Figure 10: Length of Myocardial Bridge.
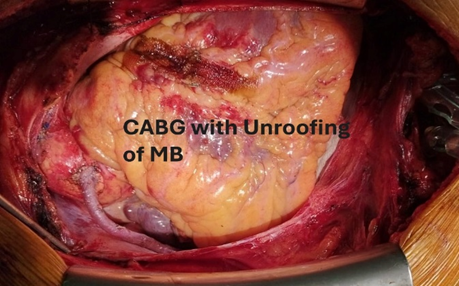
Figure 11: After completion of procedure.
To reduce and/or manage any bleeding (venous or muscular) from both sides of the myotomy edges, we employed over-and-over eversion sutures with 6/0 prolene, when patient was under cardiopulmonary bypass with full heparinization. The aortic cross clamp was removed. Proximal anastomosis was done on aorta with 6/0 prolene using side biting clamp. The patient was gradually weaned from cardiopulmonary bypass. After decannulation, heparin was reversed. After maintaining proper hemostasis, wound was closed in layers keeping two mediastinal drain tubes in situ. Patient was shifted to Cardiothoracic ICU with stable hemodynamic. He was extubated on 1st post-operative day and subsequent post-operative period was uneventful. Echocardiography was done on 1st post operative day showed preserved biventricular function. Patient was discharged from the hospital on the 7th day after surgery.
Follow Up
At the one month, three months, six months and one year follow-up, the patient was doing well with free of symptoms.
Discussion
Myocardial bridge is a congenital heart condition where a segment of a coronary artery tunnels through the heart muscle (myocardium) instead of resting on its surface. The coronary artery can be divided into three segments due to the presence of the myocardial bridge: proximal, underneath and distal to the myocardial bridge [15]. As a result, the external pressure of the myocardial fibers on the coronary artery wall can cause certain arterial segments to significantly reduce in diameter during ventricular contraction in systole. This phenomenon is referred to as the "milking effect”. Therefore, ischemic-related problems could arise from this systolic phenomenon alone. Moreover, myocardial bridge-induced turbulent coronary blood flow, coronary blood flow alterations and axial stretch of the artery wall can all contribute to the development of accelerated atherosclerosis in the coronary segment directly proximal to the bridge’s segment [16].
Classification of myocardial bridges proposed by Schwarz et al., in the absence of coronary artery disease: (a) Type A - clinical symptoms and no objective signs of ischemia (b) Type B - clinical symptoms and objective signs of ischemia by noninvasive stress testing and (c) Type C - clinical symptoms and objective abnormal intracoronary hemodynamics (by quantitative coronary assessment/coronary flow reserve/intracoronary Doppler) [17]. The middle segment of the left anterior descending (LAD) coronary artery is where myocardial bridging most frequently occurs (77.2%). Then it occurs in left circumflex artery (40%) and the right coronary artery (36%) [8]. Moreover, on histology, diagonal (18%) and marginal (40%) branches are also involved [18]. Typical myocardial bridge was reported on depth at 1-10 mm, with length of 10-30mm [19]. The prevalence of myocardial bridge during coronary angiography ranges from 0.5% to 16% [20]. In a survey of 35,000 patients referred for coronary angiography between June 2012 and June 2020, Matta et al. found that 1.42% of the study population had myocardial bridge of lt. anterior descending artery (LAD) [21]. In Bangladesh, the incidence of myocardial bridge among cardiovascular patients is unknown due to lack of medical records, shortage of modern diagnostic tools and lack of patient awareness about coronary artery disease.
Systolic narrowing at myocardial bridging segment causes mechanical stress that may damage endothelium. This can then lead to platelet aggregation, coronary vasospasm, and acute coronary syndrome. Alternative causes of ischemia include endothelial dysfunction, vasospasm, and atherosclerotic processes that develop in the proximal portion of the bridging segment of the affected artery. Diagnostic tools of myocardial bridges include Coronary angiography (CAG), multislice CTA, intracoronary ultrasound (IVUS), Fractional flow reserve (FFR), Cardiac Magnetic Resonance Imaging (CMRI). But Coronary angiography (CAG) is the most common and gold standard to diagnose myocardial bridge.
Coronary angiography (CAG) shows signs of myocardial ischemia compressed by myocardial bridges during systole (milking effect), while the coronary artery compression is relieved during diastole. Fractional flow reserve (FFR) is helpful to assess the physiology and hemodynamics of a bridging segment. IVUS is indicated when angiographically significant “milking effect” is absent with coronary provocation test [22]. Computed tomography angiography (CTA) is valuable tool for direct visualization of coronary arteries anatomy and patency with surrounding tissue and to detect only minimal or no systolic compression or any change in the vessel course occurs at the bridge segment [23]. Cardiac MRI determines whether the coronary artery blood supply function at the myocardial bridge is abnormal and displays the relationship between the mural coronary and myocardial bridge. Atherosclerosis may develop in association with myocardial bridging in same coronary artery proximal to the bridging segment, or atherosclerosis of one coronary artery with or without myocardial bridging of another coronary artery.
First line therapy of symptomatic myocardial bridge is medical treatment with beta blockers and calcium channel blockers except nitrates are contraindicated due to increase in heart rate and worsen symptoms. PCI with drug-eluting stents may be indicated in severely symptomatic patients who are refractory to medical treatment and who are not fit for surgery. Stent related complications such as coronary perforation occurs in 6
Conclusion
Myocardial bridge is a congenital malformation on the affected coronary artery. It is associated with several cardiovascular problems, including myocardial ischemia, heart attack, arrhythmia, even sudden cardiac arrest, and death. Surgical unroofing with coronary artery bypass grafting is a safe and effective treatment for symptomatic isolated myocardial bridge and or concomitant with other coronary artery disease where other options are failed, to improve coronary perfusion, relieve myocardial ischemia and improve the quality of life of the patients by relieving the compression of tunneled artery.
Declarations
Acknowledgments
Not Applicable
Conflicts of Interest
The authors declare that there are no conflicts of interest.
Funding
None.
Ethics
Written informed consent was obtained from the patient.
Consent to Participate
The work was approved by all the authors for participation.
References
- Akdemir, R., Gunduz, H., Emiroglu, Y., Uyan, C. (2002). Myocardial Bridging as a Cause of Acute Myocardial Infarction: A Case Report. BMC Cardiovascular Disorders, 2:1-5.
Publisher | Google Scholor - Reyman, H. C. (1737). Dissertation on The Proper Vessels of The Heart. Med Diss Univ, Gottingen.
Publisher | Google Scholor - Ki, Y. J. (2021). Myocardial Bridging Presenting as Myocardial Ischaemia Induced Cardiac Arrest: A Case Report. BMC Cardiovascular Disorders, 21:1-6.
Publisher | Google Scholor - Kwan, B., Singh, A. (2022). Acute Coronary Syndrome Caused by Myocardial Bridging. The American Journal of Emergency Medicine, 52:272-e1.
Publisher | Google Scholor - HC, R. (1737). Dissertation on The Proper Vessels of The Heart (Dissetation). Bib1 Anat. 2:359-379.
Publisher | Google Scholor - Porstmann, W., Iwig, J. (1960). The Intramural Coronary Angiogram. In RöFo-Fortschritte im Bereich der Röntgenstrahlen und der Imagingverfahren. 92(2):129-133.
Publisher | Google Scholor - Kawai, H., Ohta, M., Motoyama, S., Hashimoto, Y., Takahashi, H., et al. (2020). Computed Tomographic Angiography-Verified Myocardial Bridge and Invasive Angiography-Verified Left Anterior Descending Coronary Artery Vasospasm. Cardiovascular Interventions, 13(1):144-146.
Publisher | Google Scholor - Çiçek, D., Kalay, N., Muderrisoglu, H. (2011). Incidence, Clinical Characteristics, and 4-Year Follow-Up of Patients with Isolated Myocardial Bridge: A Retrospective, Single-Center, Epidemiologic, Coronary Arteriographic Follow-Up Study in Southern Turkey. Cardiovascular Revascularization Medicine, 12(1):25-28.
Publisher | Google Scholor - Ferreira, A. G., Trotter, S. E., König, B., Decourt, L. V., Fox, K., et al. (1991). Myocardial Bridges: Morphological and Functional Aspects. Heart, 66(5):364-367.
Publisher | Google Scholor - Angelini, P., Trivellato, M., Donis, J., Leachman, R. D. (1983). Myocardial Bridges: A Review. Progress in Cardiovascular Diseases, 26(1):75-88.
Publisher | Google Scholor - Nakaura, T., Nagayoshi, Y., Awai, K., Utsunomiya, D., Kawano, H., et al. (2014). Myocardial Bridging is Associated with Coronary Atherosclerosis in The Segment Proximal to The Site of Bridging. Journal of Cardiology, 63(2):134-139.
Publisher | Google Scholor - Lee, M. S., Chen, C. H. (2015). Myocardial Bridging: An Up-to-Date Review. The Journal of Invasive Cardiology, 27(11):521.
Publisher | Google Scholor - Hemmati, P., Schaff, H. V., Dearani, J. A., Daly, R. C., Lahr, B. D., et al. (2020). Clinical Outcomes of Surgical Unroofing of Myocardial Bridging in Symptomatic Patients. The Annals of Thoracic Surgery, 109(2):452-457.
Publisher | Google Scholor - Tarantini, G., Migliore, F., Cademartiri, F., Fraccaro, C., Iliceto, S. (2016). Left Anterior Descending Artery Myocardial Bridging: A Clinical Approach. Journal of the American College of Cardiology, 68(25):2887-2899.
Publisher | Google Scholor - Möhlenkamp, S., Hort, W., Ge, J., Erbel, R. (2002). Update on Myocardial Bridging. Circulation, 106(20):2616-2622.
Publisher | Google Scholor - Klues, H. G., Schwarz, E. R., vom Dahl, J., Reffelmann, T., Reul, H., et al. (1997). Disturbed Intracoronary Hemodynamics in Myocardial Bridging: Early Normalization by Intracoronary Stent Placement. Circulation, 96(9):2905-2913.
Publisher | Google Scholor - Schwarz, E. R., Gupta, R., Haager, P. K., Vom Dahl, J., Klues, H. G., et al. (2008). Myocardial Bridging in Absence of Coronary Artery Disease: Proposal of a New Classification based on Clinical-Angiographic Data and Long-Term Follow-Up. Cardiology, 112(1):13-21.
Publisher | Google Scholor - Möhlenkamp, S., Hort, W., Ge, J., Erbel, R. (2002). Update on Myocardial Bridging. Circulation, 106(20):2616-2622.
Publisher | Google Scholor - Angelini, P., Trivellato, M., Donis, J., Leachman, R. D. (1983). Myocardial Bridges: A Review. Progress in Cardiovascular Diseases, 26(1):75-88.
Publisher | Google Scholor - Karna, S. K., Chourasiya, M., Parikh, R. P., Chaudhari, T., Patel, U. (2020). Prevalence of Myocardial Bridge in Angiographic Population-A Study from Rural Part of Western India. Journal of Family Medicine and Primary Care, 9(4):1963-1966.
Publisher | Google Scholor - Matta, A., Canitrot, R., Nader, V., Blanco, S., Campelo-Parada, F., et al. (2021). Left Anterior Descending Myocardial Bridge: Angiographic Prevalence and Its Association to Atherosclerosis. Indian Heart Journal, 73(4):429-433.
Publisher | Google Scholor - Ge, J., Erbel, R., Rupprecht, H. J., Koch, L., Kearney, P., et al. (1994). Comparison of Intravascular Ultrasound and Angiography in The Assessment of Myocardial Bridging. Circulation, 89(4):1725-1732.
Publisher | Google Scholor - Leschka, S., Koepfli, P., Husmann, L., Plass, A., Vachenauer, R., et al. (2008). Myocardial Bridging: Depiction Rate and Morphology at CT Coronary Angiography-Comparison with Conventional Coronary Angiography. Radiology, 246(3):754-762.
Publisher | Google Scholor - Ernst, A., Bulum, J., Šeparović Hanževački, J., Lovrić Benčić, M., Strozzi, M. (2013). Five-Year Angiographic and Clinical Follow-Up of Patients with Drug-Eluting Stent Implantation for Symptomatic Myocardial Bridging in Absence of Coronary Atherosclerotic Disease. J Invasive Cardiol, 25(11):586-592.
Publisher | Google Scholor - Tandar, A., Whisenant, B. K., Michaels, A. D. (2008). Stent Fracture Following Stenting of a Myocardial Bridge: Report of Two Cases. Catheterization and Cardiovascular Interventions, 71(2):191-196.
Publisher | Google Scholor - Jiang, Q., Liang, C., Wu, Z. (2012). Myocardial Bridging is a Potential Risk Factor of Very Late Stent Thrombosis of Drug Eluting Stent. Medical Science Monitor: International Medical Journal of Experimental and Clinical Research, 18(5):HY9.
Publisher | Google Scholor - Mok, S., Majdalany, D., Pettersson, G. B. (2019). Extensive Unroofing of Myocardial Bridge: A Case Report and Literature Review. SAGE Open Medical Case Reports, 7:2050313X18823380.
Publisher | Google Scholor - Al-Musawi, M., Marsh, A., Yi, S., AlOmaishi, S., Rubay, D., et al. (2019). Combined Myocardial Bridge and Coronary Vessel Disease Requiring Coronary Artery Bypass Grafting and Myotomy of the Myocardial Bridge. Cureus, 11(12).
Publisher | Google Scholor























